

-

Squashing Superbugs: Using Procalcitonin Levels toIdentify Bacterial Infections to Direct Antibiotic Therapy
Janna Berg, Tera Holland, and Krista Westbrook
The current standard in diagnosing and treating pediatric infections is obtaining cultures, interpreting complete blood count results, and following the trends of erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). Infection triggers an inflammatory response; if untreated or mistreated, this microbe invasion can lead to sepsis. The purpose of this submission is to address the promising use of procalcitonin levels (PCT) as a superior marker in the early detection of bacterial infection via a scholarly literature review.
Studies involving PCT are more readily found in the evaluation of the neonatal population and in adults with respiratory illnesses. Pediatric studies are limited, therefore more research and an increased number of subjects are needed to validate PCT as being the best marker for early bacterial detection. PCT levels in a healthy individual are almost undetectable and will rise sharply when the inflammatory response is triggered by invading bacteria. PCT levels normalize faster than CRP levels in response to appropriate therapy; antibiotic therapy can be individualized to match this recovery. ESR and CRP do not differentiate bacterial infections from other invaders thus a predetermined antibiotic course is indiscriminately prescribed. The literature explains that PCT levels could encourage prompt diagnosis, early treatment and antibiotic stewardship.
A scholarly search of more than 30 journal articles was reviewed and critiqued by the presenters. Research shows that in adults and neonates, PCT is the standard for diagnosing and treating bacterial infections. Elevated PCT levels in neonates determine the need for antibiotic treatment in bacterial infection or supportive treatment in its absence (viral infection). Determining the nature of increased inflammation is crucial to treatment; it can help isolate infections in adults presenting with pre-existing respiratory diseases, like COPD. Studies on the pediatric population show promise that PCT will be just as crucial in bacterial infections.Levy, H., & Sayegh, M. (2019). Procalcitonin testing as an aid to antibiotic stewardship. Medical Laboratory Observer, 51(9). https://www.mlo-online.com/disease/antibiotic-resistance/article/21093254/procalcitonin-testing-as-an-aid-to-antibiotic-stewardship
Memar, M. Y., Varshochi, M., Shokouhi, B., Asgharzadeh, M., & Kafil, H. S. (2017). Procalcitonin: The marker of pediatric bacterial infection. Biomedicine & Pharmacotherapy, 96, 936-943. DOI:10.1016/j.biopha.2017.11.149
Poddar, B., Gurjar, M., Singh, S., Aggarwal, A., & Baronia, A. (2016). Reduction in procalcitonin level and outcome in critically ill children with severe sepsis/septic shock--A pilot study. Journal of Critical Care, 36, 230-233. DOI: 10.1016/j.jcrc.2016.07.022
Trippella, G., Galli, L., Martino, M. D., Lisi, C., & Chiappini, E. (2017). Procalcitonin performance in detecting serious and invasive bacterial infections in children with fever without apparent source: A systematic review and meta- analysis. Expert Review of Anti-infective Therapy, 15(11), 1041-1057. DOI:10.1080/14787210.2017.1400907Vijayan, A. L., Vanimaya, Ravindran, S., Saikant, R., Lakshmi, S., Kartik, R., & G, M. (2017). Procalcitonin: A promising diagnostic marker for sepsis and antibiotic therapy. Journal of Intensive Care, 5(1). DOI:10.1186/s40560-017-0246- 8
-

Improving Catheter Associated Urinary Tract Infection Rates ofPediatric Patients Through Standardization of Catheter Care
Shelby Beyers, Jenna Buys, and Hayden Dutton
Background/Significance: Pediatric patients with urinary catheters are at an increased risk for developing Catheter Associated Urinary Tract Infections (CAUTI). Standardization of urinary catheter care improves CAUTI rates. At Children’s Health, the CAUTI rate increased from 2 infections to 10 infections from 2018 to 2019. Review of organizational policy revealed that urinary catheter care practices were not standardized. Bedside staff performed catheter care with soap and water but utilized different methods and supplies, leading to variability in practice.
Purpose/EBP Question: The purpose of this Evidence Based Practice (EBP) project was to standardize catheter care throughout Children’s Health. Nurse resident sought to answer if the use of meatal and perineal cleansing cloths in comparison to current standard of care with soap water reduced the incidence of CAUTIs at a large pediatric health system.
Implementation Plan/Methods: The CAUTI Committee trialed meatal and perineal cleansing cloths beginning in January 2020. During the trial, the nursing staff were surveyed regarding the ease and efficiency of the cleansing cloths.
Results/Outcomes: Standardization of urinary catheter care, improved CAUTI rates in 2020. The organization observed a decrease in the mean CAUTI rate from 2.0 in 2019 (N=10) to a mean rate of 0.3 in 2020 (N=1) after trialing and implementing the urinary catheter cleansing cloths. Staff surveys from the product trials provided positive feedback. Staff appreciated the convenience and efficiency of the wipes as well as the additional instructions provided on the inside of the packaging. Use of the cleansing cloths led to a 90% reduction in CAUTIs resulting in an estimated cost savings of $90K for this organization.
Conclusions/Implications for Practice: Use of catheter cleansing cloths are an effective strategy to standardize catheter care, decrease costs, and improve CAUTI rates in pediatric patients
-

Improving Pediatric Healthcare Workers Personal Safety Through the Implementation of a Behavioral Rapid Response Team
Jennifer Brown and Diana Montoya
From 2017 to 2018, a metropolitan pediatric hospital noted a 62.6% increase in calls to security for uncooperative patients related to physical aggression and acute behavioral decompensation. Even with annual de-escalation and restraint training, a 2019 survey conducted by clinical educators discovered only 27% of staff felt safe when handling an aggressive patient. This drove a collaborative initiative to formulate a multidisciplinary Behavioral Emergency Response Team (BERT) to standardize care, emergently respond in behavioral situations, and act as a resource to staff. Nurse professional development (NPD) specialists were used to create and develop a multifaceted education approach including instructor-led training, simulation, a computer-based training program and a six-month post-implementation face-to-face content refresher and simulation. One-year post implementation, and over 100 BERT responses, a follow up survey revealed staffs’ perception of personal safety more than doubled to 55%. This illustrates the BERT is a valuable staff resource and supports a safer work environment. Continuous tracking of BERT activations, responses, and staff perceptions of personal safety will help fine tune the current process and allow for development of future programs to promote workplace safety. The success in development, training and implementation of the BERT on our main campus, has led to its adoption at other satellite hospitals.
-

Promoting Patient Safety using Virtual Safety Huddles
Rachael Burris-Alcala, Julie Baker, and Ann Gosdin
Background: Staff Safety Huddles have been shown to improve communication and to help make patient safety a priority. Conducting daily safety huddles in Plano ACS are difficult because of how each nursing unit is structured. There are four units with 12 beds in each unit. The units are separated from each other and only have one charge nurse for all four units. Finding a solution to conduct daily huddles was a priority. Safety huddles occurred daily on both day and night shifts. Although the safety huddles helped identify safety concerns, it did not solve the problem of the entire department "huddling" together at one unified time to identify safety concerns.
Methods: Safety Huddles were trialed in a virtual forum. The virtual forum was done in collaboration with the virtual health team. The virtual model allows all four units to discuss safety events for their shift all together at one time.
Results: Safety Huddles began in March 2021 in person to get staff used to having huddles. Then we switched to a virtual model in April 2021.
The following safety issues were identified during Virtual Safety Huddles:
- 59 Patient safety concerns were expressed by staff and addressed proactively.
- 12 Medication safety concerns were expressed and resolved in collaboration with Pharmacy and ACS for medication delivery accuracy.
- 5 Clinical informatics/EPIC tools request were made to address concerns.
- 9 Engineering and Equipment requests were made.
- 1 Clinical Education request submitted
- 1 Patient Education submitted
Additionally, a RISE consult was made to support staff needs.
Conclusion: Virtual Safety Rounds were helpful in improving communication and help proactively address safety concerns of staff.
-

IR Unplanned Line Removals
Toni Haynes
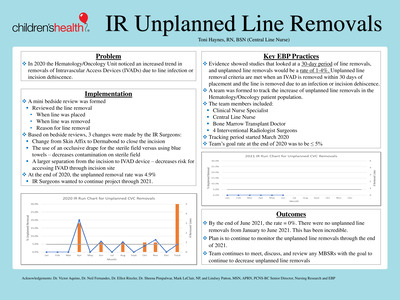
Problem
In 2020, the Hematology/Oncology unit noticed an increased trend in Intravascular Access Devices (IVADs) needing to be removed due to infection or dehiscence of the incision.Key EBP Practices
A Clinical Nurse Specialist, Central Line Nurse, Bone Marrow Transplant Doctor, and four Interventional Radiologist Surgeons came together to discuss potential causes of the increase in line removals. Team decided to track unplanned line removals. Unplanned line removal criteria are met when a central line is removed within 30 days of placement from an infection or dehiscence. Evidence shows studies looked at 30-day periods for line removals, and line removals would be as low as 1-4 percent.Implementation/Pilot Testing
Project started in 2020. Goal rate for the end of the year was to be less than or equal to 5 percent. At the end of 2020, the unplanned removal rate was 4.9%. Due to barely meeting the goal, the project will continue in 2021. A mini bedside review (BSR) was completed with every unplanned line removal. The BSR reviewed when the line was placed, removed, and the reason. BSR’s were discussed by the team to find potential causes for removals. Three changes were made by the surgeons: change from Skin Affix to Dermabond to close the incision, the use of an occlusive drape for the sterile field versus blue towels, and a larger separation from the incision to IVAD device.Outcomes
By the end of June 2021, the rate equaled 0%. There were no unplanned line removals from January to June. This has been incredible. The plan is to continue to monitor the unplanned line removals through the end of 2021. -

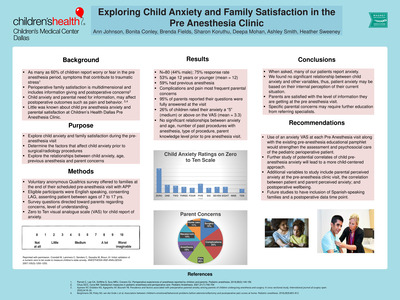
Exploring Child Anxiety and Family Satisfaction in thePre Anesthesia Clinic
Ann Johnson, Bonita Conley, and Brenda Fields
Studies show that families experience anxiety in the perioperative period. From the child’s perspective, coping with stressful experiences varies according to their appraisal of the situation, their experience and cognitive stage. Child stress or anxiety is best ascertained by self-report, and there is lack of evidence about the child's perspective during the pre-anesthesia period, as well as factors that relate to child anxiety. Purpose: The purpose of this project was to explore child report of anxiety during the pre-anesthesia clinic visit prior to a scheduled procedure with general anesthesia in a sample of patients ages 7 to 17 years. We also aimed to explore relationships between child anxiety, age, previous anesthesia, and parent concerns. Methods: A voluntary survey via Qualtrics was offered to English-speaking consenting families at the end of their scheduled pre-anesthesia visit at a pediatric specialty center affiliated with a regional hospital in the south central United States. The survey included the Zero to Ten visual analogue scale (VAS) for child report of anxiety. Results: Preliminary analysis of the first 70 participants revealed near 50% age 12 years or younger, approximately 30% rated their anxiety a “5” (medium) or above on the VAS (mean = 3.1), and there was almost no relationship between age and anxiety (r= 0.02). There was a small negative correlation between child anxiety and number of past procedures with anesthesia (r= -0.1) and a small positive correlation between child anxiety and parents getting all of their questions answered during the visit (r=0.2). Limitations include exclusion of Spanish-speaking families (this is a large population at our clinic). Among implications for practice is the presence of anxiety in pre- anesthesia clinic patients of all ages, especially those with less anesthesia experience. Conclusion: Use of an anxiety VAS would strengthen the assessment and psychosocial care of the pediatric perioperative patient. Further study of potential correlates of child pre-anesthesia anxiety will lead to a more child-centered approach.
-

How a Crew of Experts Can Pave the Road to Quality Improvement inPreventing Central Line-Associated Bloodstream Infections
Ginny Leinweber, Angie Morris, and Kendra Shotts-Fraser
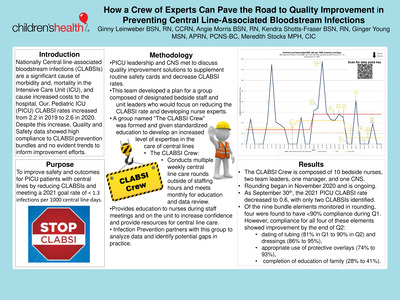
Purpose
To improve outcomes for PICU patients with central lines by reducing central line-associated bloodstream infections (CLABSIs) and meeting a 2021 goal rate of < 1.3 infections per 1000 central line days.
Background
PICU CLABSI rates increased from 2.2 in 2019 to 2.6 in 2020. Despite this increase, Quality and Safety data showed high compliance to CLABSI prevention bundles and no evident trends to inform improvement efforts.
Methodology
PICU leadership and CNS met to discuss quality improvement solutions to supplement routine safety cards and decrease CLABSI rates. This team developed a plan for a group composed of designated bedside staff and unit leaders who would focus on reducing the CLABSI rate and developing nurse experts. The group named the CLABSI Crew was formed with a charter outlining the purpose, team member responsibilities, rounding logistics, and expected outcomes. The CLABSI Crew conducts 12 hours of weekly central line care rounding outside of staffing hours and meets monthly for education and data review. The CLABSI Crew also provides education to nurses during staff meetings and on the unit to increase confidence and provide resources for central line care. Infection Prevention partners with this group to analyze data and identify potential gaps in practice.
Results
The CLABSI Crew is composed of 10 bedside nurses, two team leaders, one manager, and one CNS. All members received additional central line training. Rounding began in November 2020 and is ongoing. As of the end of Q2, the 2021 PICU CLABSI rate decreased to 0.5, with only one infection identified. Of the nine bundle elements monitored in rounding, four were found to have <90% compliance during Q1. However, compliance for all four of these elements showed improvement by the end of Q2: dating of tubing (81% in Q1 to 90% in Q2) and dressings (86% to 95%), appropriate use of protective overlays (74% to 93%), and completion of education of family (28% to 41%).
-

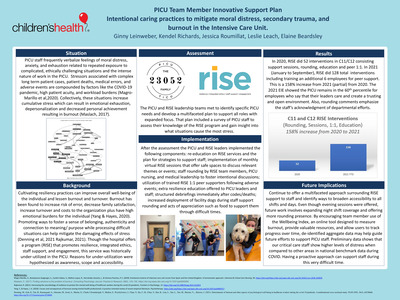
PICU Team Member Innovative Support PlanIntentional caring practices to mitigate moral distress, secondary trauma, andburnout in the Intensive Care Unit.
Ginny Leinweber, Kendel Richards, and Jessica Roumillat
Situation:
PICU staff frequently verbalize feelings of moral distress, anxiety, and exhaustion related to repeated exposure to complicated, ethically challenging situations and the intense nature of work in the PICU. Stressors associated with complex long term patient cases, deaths, medical errors, and adverse events are compounded by factors like the pandemic, high patient acuity, and instability of staffing. Collectively, these situations increase the risk of burnout and decreased job satisfaction.
Background:
Research shows that cultivating resiliency practices can improve overall well-being of the individual and lessen burnout and turnover. Though the hospital offers a program (RISE) that promotes resilience, integrated ethics, staff support, and engagement this service was historically under-utilized in the PICU.
Assessment:
The PICU and RISE leadership team met to identify specific PICU needs and develop a multifaceted plan to support staff. That included a survey of PICU staff to assess their knowledge of the RISE program and gain insight into what situations cause the most stress.
Implementation:
After the assessment, the PICU and RISE leaders implemented the following components: re-education on RISE services and the plan for strategies to support staff; implementation of monthly RISE sessions that offer safe spaces to discuss relevant themes or events; staff rounding by RISE and PICU leadership to foster intentional discussions; utilization of trained RISE 1:1 peer supporters following adverse events; resilience education offered to PICU leaders and staff; structured debriefings immediately after codes/deaths; increased dog rounding and acts of appreciation such as food or personalized notes.
Results:
Since implementation, the PICU has offered 30 RISE sessions impacting 194 employees, supported 59 employees through 1:1 peer support, and trained 6 additional employees for peer-to-peer support. In total there has been over 360 staff personal interactions. The 2021 EIE showed the PICU remains in the 60th percentile for employees saying that leaders care and create a trusting and open environment. Also, rounding comments emphasize the staff’s acknowledgment of departmental efforts to support them through difficult times.
-
 by Katie McLaurin")
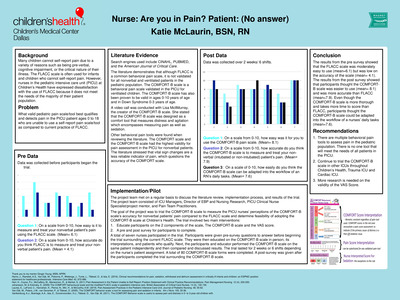
Nurse: Are you in Pain? Patient: (No answer)
Katie McLaurin
Many infants and children admitted to the pediatric intensive care unit (PICU) have difficulty self-reporting pain requiring nurses to score pain utilizing the FLACC scale. However, when surveyed, PICU nurses at Children’s Health expressed dissatisfaction with the FLACC scale because it did not accurately assess pain in the PICU population (mean=4.1). An extensive literature review was conducted to determine the best behavioral pain scale to use for nonverbal patients in the PICU. Based on the literature, the COMFORT-B scale was selected. The COMFORT-B scale is a behavioral pain scale validated in the PICU in children 0 to 10 years and in Down Syndrome 0 to 3 years. The goal of the project was to trial the COMFORT-B Scale to measure the PICU nurses’ perceptions of the COMFORT-B scale’s accuracy for non-verbal patients’ pain compared to the FLACC scale and determine feasibility of adopting the COMFORT-B scale at Children’s Health. Seven PICU nurses participated in the trial. Following education of the COMFORT-B scale, nurses scored their patients with the tool over two weeks on 80 patients. Participants completed a pre and post survey questions. The results from the post survey showed at participants thought the COMFORT-B scale was easier to use (mean= 8.1) and was more accurate (mean= 7.9) than FLACC. Even though the COMFORT-B scale is more thorough and takes more time to score than FLACC, participants thought the COMFORT-B Scale could be adapted into the workflow of a nurse’s daily tasks (mean=7.6).
-
PATIENT QUESTIONNAIRE INPLEMENTED AT CHILDREN’S HEALTH by Jane Miles, Karla Hutcherson, and Jennifer Brown")
INITIAL RESULTS OF THE ASQ (ASK SUICIDE QUESTIONS)PATIENT QUESTIONNAIRE INPLEMENTED AT CHILDREN’S HEALTH
Jane Miles, Karla Hutcherson, and Jennifer Brown
OBJECTIVE
Our goal was to assess the outcome of recently implemented hospital wide questionnaire ,Ask suicide Screening Questions (ASQ), for all patients seen at Children’s Health ER from April to December 2018.
BACKGROUND
Suicide is the second leading cause of death in youth ages 10-24 and is a significant public health problem. Early identification and treatment can have an impact on the number of youth suicides.
METHOD
Due to demand, a specific workflow was created and implemented hospital wide. ASQ questionnaire consists of 5 questions. If patient answers “no” to first four questions, the fifth question is not asked. If the answer is “yes” to any of the questions or if the patient refuses to answer, a fifth question is asked. Positive ASQ result is followed by a full mental health and safety assessment, and implementation of suicide precautions. Parents/guardians answer the questions for youth 6-9 regarding history of suicidal behaviors or concerns they may have for the child’s safety. Again, a positive answer to any question triggered further assessment and appropriate referrals.
Authors have done retrospective ASQ data review. The data are secured on the Hospital server and protected by password. The project got IRB approval.
The data was examined by descriptive analysis and simple graphic focusing on demographics, chief complaint (Suicidal Ideations or Attempt), previous history of suicide, insurance and follow up treatments.
RESULTS
Number of patients seen in Dallas ER in period between April-December 2018 was 3714; 1900 patients were between ages 6-9 and 2213 between ages 10-18.
In the younger age group 1.05% of total patients seen reported suicidal ideations or suicide attempts. In the older age group 17.75% patients reported suicidal ideations or have attempted suicide. Majority of patients seen in both groups received treatment (inpatient or outpatient follow up)
CONCLUSION
Implementation of ASQ helps to detect suicidal ideations in patient who present to ER.
-

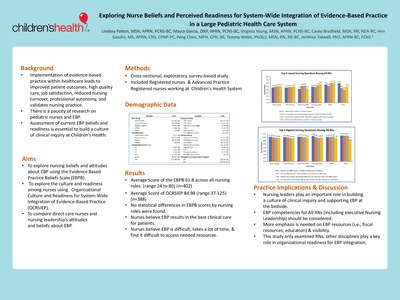
Exploring Nurse Beliefs and Perceived Readiness for System-Wide Integration of Evidence-Based Practice in a Large Pediatric Health Care System
Lindsey Patton, Mayra Garcia, Virginia Young, and Jerithea Tidwell
Background: Implementation of evidence-based practice within healthcare leads to improved patient outcomes, high quality care, job satisfaction, reduced nursing turnover, professional autonomy, and validates nursing practice. Although there is a plethora of research focusing on implementation of EBP, little attention has been given to assess organizational readiness for integration.
Aims/ Methods: The primary aims were to explore nursing beliefs and attitudes about EBP using the Evidence Based Practice Beliefs Scale (EBPB) and the culture and readiness among pediatric nurses for system wide integration of EBP using the Organizational Culture and Readiness for System-Wide Integration of Evidence-Based Practice (OCRSIEP).
Results: Overall pediatric nurses had an average score of 61.8 (SD on the EBPB (N=396). No statistical differences in EBPB scores by nursing roles were found, however, nursing leaders had higher scores than any other nursing role. The OCRSIEP had an average score of 84.98 (N=388).
Discussion: Overall, findings suggest that pediatric nurses believe that EBP results in the best clinical care for patients and that it can improve clinical care, but they lack the skills and time necessary to engage in the process.
Practice Implications: Developing EBP competencies may assist in preparing pediatric nurse leaders and front-line staff with integration of EBP into daily practice. This may positively impact organizational readiness by increasing confidence and intentionality needed to remove identified barriers and engrain EBP in the organization’s culture.
-

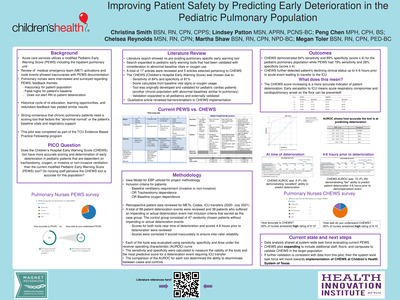
Improving Patient Safety by Predicting Early Deterioration in thePediatric Pulmonary Population
Christina Smith, Lindsey Patton, and Peng Chen
Background: The inpatient pulmonary unit (D9) utilizes a modified pediatric early warning score (PEWS) to identify deteriorating patients. D9 emergency team activations and code event reviews found PEWS documentation discrepancies and inaccuracies. 66% of D9 nurses reported PEWS scores are inaccurate for the pulmonary population and this is a major barrier to using PEWS. The Iowa model was used to identify a different tool, compare psychometrics, and measure nurses’ perceptions to establish the best early warning tool for pediatric pulmonary patients.
Methods: Inclusion criteria was patients admitted to D9 with baseline tracheostomy, oxygen, or invasive/non-invasive ventilation. Literature review revealed no pre-existing pediatric pulmonary specific early warning tool. However, the Children’s hospital early warning score (CHEWS) tool is validated with 84% sensitivity and 81% specificity and utilizes patient’s baseline status; thus, practice change was recommended to use CHEWS. Nurses completed a CHEWS paper pilot form on patients who met inclusion criteria, these patients were the “control” group and did not experience deterioration events. Retrospective chart analysis was completed on all D9 deterioration events and ICU transfers for the past 18 months. CHEWS and PEWS scores at time of event and 4-6 hours prior to event were analyzed. Nursing perception survey of PEWS and CHEWS was obtained.
Results: The pilot results yielded 38 patient deterioration events and 47 control events. CHEWS score demonstrated 84% sensitivity and 89% specificity while PEWS sensitivity was 79% and specificity was 28% showing PEWS failed to be an accurate predictor of deterioration and ICU transfer. CHEWS pilot has now expanded across Children’s Health System of Texas, which will balance some of the initial pilot concerns of high census, high unit acuity, and small sample size. Additional sensitivity and specificity will be calculated from the larger group for validation, if validation is consistent with pilot then CHEWS tool will be implemented.
-

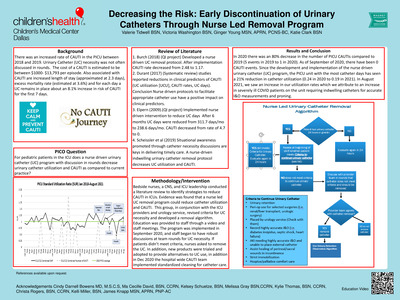
Decreasing the Risk: Early Discontinuation of UrinaryCatheters Through Nurse Led Removal Program
Valerie Tidwell, Victoria Washington, and Ginger Young
Purpose- Improve outcomes and safety for PICU patients through an Evidence Based Practice (EBP) approach to reduce catheter associated urinary tract infections (CAUTI)
PICO For pediatric patients in the ICU does a nurse driven urinary catheter (UC) program with discussion in rounds decrease urinary catheter utilization as compared to current practice?
Background There was an increased rate of CAUTI in the PICU between 2018 and 2019. UC necessity was not often discussed in rounds. The cost of a CAUTI is estimated to be between $1000- $13,793 per episode. Also associated with CAUTI are increased LOS (approximated at 2.3 days), excess mortality rate (estimated at 3.6%) and for each day a UC remains in place about an 8.1% increase in risk of CAUTI for the first 7 days.
Methodology/Intervention A group of bedside nurses, CNS, two team leaders, and manager conducted a literature review to identify strategies to reduce CAUTI in an ICU. Evidence was found that a nurse led urinary catheter (UC) removal program could reduce catheter utilization and CAUTI. This group in conjunction with the ICU medical director, ICU providers, and urology revised criteria for UC necessity and developed a removal algorithm. Education was provided to staff through a video and meetings. The program was implemented in September 2020 and nursing staff began to have robust discussions at team rounds for UC necessity. If patients didn’t meet criteria, nurses asked to remove the UC. In addition, new products were trialed and adopted to provide alternatives to UC use.
Results
In 2020 there was an 80% decrease in the number of PICU CAUTIs compared to 2019 (5 events in 2019 to 1 in 2020). As of September of 2020, there have been 0 CAUTI events. Since the development and implementation of the nurse driven urinary catheter (UC) program, the PICU unit with the most catheter days has seen a 21% reduction in catheter utilization (0.24 in 2020 to 0.19 in 2021).
-

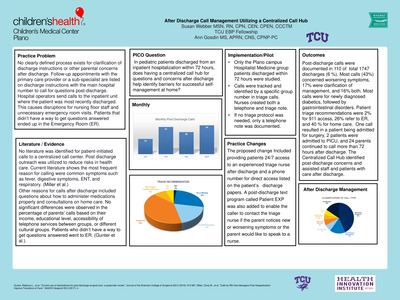
After Discharge Call Management Utilizing a Centralized Call Hub
Susan Webber and Ann Gosdin
Practice Problem
No clearly defined process exists for clarification of discharge instructions or other parental concerns after discharge. Follow-up appointments with the primary care provider or a subspecialist are listed on discharge instructions with the main hospital number to call after discharge. Hospital operators send calls to inpatient units where the patient was most recently discharged. This causes disruptions for nursing floor staff and unnecessary emergency room visits. No literature was identified for calls to a centralized call center after discharge. Literature shows the most frequent reason for calling after discharge were common concerns such as fever, ENT, respiratory and digestive symptoms.PICO Question
In pediatric patients discharged from an inpatient hospitalization within 72 hours, does having a centralized call hub for questions and concerns after discharge help identify barriers for successful self-management at home?Implementation/Pilot
Only Plano Hospitalist Medicine group patients discharged within 72 hours were studied. Calls were tracked and identified by a specific group number in triage calls. Nurses created both a telephone and triage note. If no triage protocol was needed, only a telephone note was documented.Practice Changes
Proposed changes Included providing patients a direct phone number for 24/7 access to experienced triage nurses on discharge paperwork. A post-discharge text program called Patient EXP was added to contact the triage nurse if the parent needs to speak to a nurse.Outcomes
Most calls (43%) concerned worsening symptoms, 17% were clarification of management, and 16% for both. Most calls were for newly diagnosed diabetics, followed by gastrointestinal disorders. Triage recommendations were 2% for 911 access, 26% refer to ER, and 40 % for home care. One patient was admitted for surgery. Two patients were admitted to PICU, and 24 parents continued to call 72 hours after discharge. Calls with ED or 911 a recommendation had 13% of patients readmitted. The Centralized Call Hub identified post-discharge concerns and assisted staff and patients with care after discharge.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}