

-

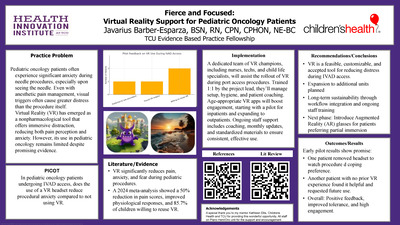
Fierce and Focused - Virtual Reality Support for Pediatric Oncology Patients
Javarius Barber-Esparza
Practice Problem: Pediatric oncology patients often experience anxiety during needle procedures. Even with anesthetic pain management in place, visually encountering the needle can be more distressing than the procedure itself. Virtual Reality (VR) has emerged as a nonpharmacological tool that provides immersive distraction, effectively lowering pain perception and anxiety. Studies show VR reduces anxiety during medical procedures, including accessing Implanted venous access devices (IVAD). Yet, its adoption in pediatric oncology settings remains limited.
Literature/Evidence: Search strategy in the CINAHL (EBSCOhost) database used MeSH headings and keywords, including English articles published within the last five years. Studies show that VR reduces pain, anxiety, and fear during procedures. A 2024 meta-analysis found VR led to 50% lower pain scores and improved physiological responses. Most children (85.7%) expressed willingness to reuse VR. Customizable programs enhance engagement and support patient-centered care. Integrating VR at the bedside addresses a gap in coping tools, aligning with ethical responsibilities to reduce trauma and improve procedural experiences.
Practice Change: This project integrates virtual reality (VR) as a standard distraction during IVAD access for pediatric oncology patients. This initiative engages pediatric hematology/oncology nurses in implementing VR to reduce procedural distress. Nurses, positioned at the intersection of technical and emotional care, play a central role in delivering this evidence-based, immersive intervention. This shift supports patient-centered care, enhances pain management, and promotes emotional safety without disrupting clinical workflow.
Implementation: A team of trained VR champions, nurses, patient care technicians, and child life specialists, will support implementation under the project lead guidance. Champions will receive 1:1 training on setup, maintenance, and patient coaching. VR will be integrated into IVAD access workflows, with age-appropriate apps selected to boost engagement. The project begins with an inpatient pilot, expanding to outpatient use. Staff engagement will be supported through debriefings, coaching, monthly updates, and standardized scripts to ensure consistent, effective implementation.
Outcomes/Results: Initial outcomes from the pilot demonstrated positive patient responses to VR use during IVAD access. One patient removed the headset prior to the procedure, expressing a desire to visually observe the process, highlighting the importance of patient autonomy and individual coping styles. Another patient, who had no prior VR experience, reported that the procedure felt better with VR and expressed willingness to use it again. Early observations suggest that VR can enhance procedural tolerance and support varied patient preferences, reinforcing its value as a customizable, patient-centered intervention.
Recommendation/Conclusion: Early results support the feasibility and acceptability of VR as a nonpharmacological strategy for reducing distress during IVAD access in pediatric oncology patients. The intervention will be expanded to additional pediatric units, with long-term sustainability supported by integrating VR into routine workflows and providing ongoing training and refresher sessions for staff. Future phases of this initiative will explore the use of augmented reality (AR) glasses for patients who prefer to remain partially engaged with their environment rather than fully immersed. This next step aims to broaden accessibility and accommodate a wider range of patient coping preferences, further advancing emotionally supportive, patient-centered procedural care. -

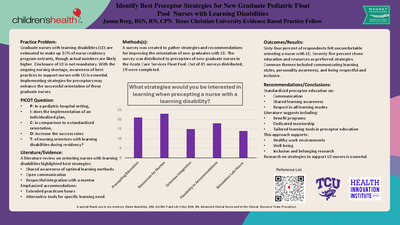
Increasing Clinical Internal Mobility Through a Student Nurse Technician Program
Radiance G. Bean
Practice Problem: Currently 67% of internal applicants are hired into our nurse residency program. Feedback from nursing leadership suggests internal candidates often fall short in areas like interviewing skills and professionalism, making external candidates stronger. Given the higher education resources provided to team members and our organization’s commitment to internal mobility, identifying ways to support employees and retaining top nursing talent is a priority. Our EBP question is: Will participation in a Student Nurse Technician (SNT) program increase the percentage of Patient Care Technicians (PCTs) in good standing that are accepted into the nurse residency compared to the current process.
Literature/Evidence: Using CINAHL Ultimate, search criteria included key word search terms: nurse apprenticeships, nurse assistant roles, recruitment and retention of Unlicensed Assistive Personnel. A review of the literature, focusing on pre-pandemic studies to eliminate COVID-related compounding variables, shows that structured support programs can improve outcomes. Studies confirm that participation in SNT programs builds loyalty and fosters recruitment success. According to Haqq-Stevens et al. (2017), academic resources were considered more valuable compared to increased skill opportunities. While Lokmic-Tomkins et al. (2021) found that institutional support leads to stronger organizational commitment and readiness to practice.
Practice Changes: To address these challenges, a Student Nurse Technician program was developed to better support nursing students working as PCTs in our Clinical Resource Team (CRT) (float pool). Participants meet monthly to discuss progress and participate in professional growth activities. The program includes three targeted components:
Academic Support: Offers NCLEX practice tests, individualized coaching, and test-taking strategy sessions, culminating in an NCLEX review course during their final semester.
Clinical Support: Provides exposure to various hospital units through shadowing, followed by debriefing conversations to help participants assess their preferences for nurse residency placement.
Professional Support: Provides feedback with resume development, mock interviews, and one-on-one interview debriefs to enhance their interview skills.
Implementation/Pilot Testing: The pilot cohort includes eight PCTs from the CRT, each having completed at least one semester of nursing school. Participants were identified via an intake form and voluntarily opted into the program. Leaders were provided with a schedule to ensure appropriate staffing and enhance flexibility.
Outcomes/Results: Outcome data will be available in December 2025. Evaluation metrics include the percentage of participants hired into the nurse residency program compared to non-participants, Casey-Fink Readiness to Practice Survey results (pre-program, in the program, and program end), and orientation duration. Literature indicates that participants in support programs typically experience shorter onboarding periods (Flint, 2023), which will be another indicator of program success.
Recommendations/Conclusions: Based on the results, the program may expand to include additional departments and campuses. There is growing interest in supporting nursing students who work in healthcare but not as PCTs, though literature suggests that best practice for SNT programming is those already in a PCT role. Barriers to scaling include inconsistent academic calendars and differing levels of participant motivation. Still, this initiative supports the broader goal of transforming internal candidates into confident, competent nursing professionals prepared for residency success. -

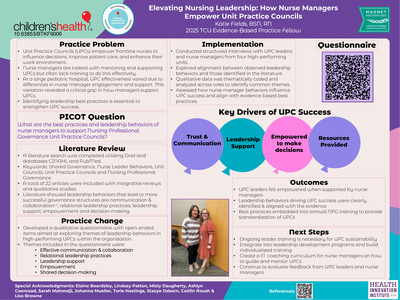
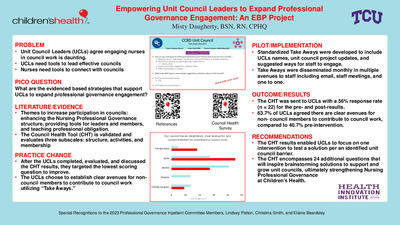
Elevating Nursing Leadership: How Nurse Managers Empower Unit Practice Councils
Katie Fields
Problem: Unit Practice Councils (UPCs) are foundational to Nursing Professional Governance (NPG), a structure that is designed to foster autonomy, accountability and authority for nurses. These councils are vital for empowering nurses to engage in decision-making and implementing practice changes. At one large pediatric hospital, UPC effectiveness varied across units, largely due to differences in nurse manager engagement and support. This variation highlighted a critical gap in how nurse managers were supporting UPCs within their unit. To close this gap, it was important to identify leadership best practices and behaviors that lead to successful UPCs. The following PICOT question was developed: “What are the best practices and leadership behaviors of nurse managers to support Nursing Professional Governance Unit Practice Councils?”
Literature/Evidence: Utilizing OVID and databases, CINAHL and PubMed, a comprehensive review of 22 articles, including integrative reviews and qualitative studies, was conducted to explore leadership behaviors that support NPG and UPCs. Across literature, empowerment, accountability, and presence are frequently highlighted as essential leadership behaviors for effective shared governance that enhances engagement and growth. Clavelle and Tarasenko (2024) emphasized accountability as key to advancing NPG, while Rollins et al. (2024) stressed the importance of adaptable leadership styles.
Practice Change: To address the variation in UPC effectiveness across units, a practice change initiative was implemented to examine whether the leadership behaviors demonstrated in high-performing UPCs aligned with those identified in the literature. The evidence highlighted key behaviors such as effective communication and collaboration, relational leadership practices, leadership support, empowerment and shared decision-making. To explore this alignment, a questionnaire was developed consisting of open-ended questions aimed at uncovering recurring themes in leadership behaviors that contribute to the success and sustainability of UPCs within the organization.
Implementation: Using the developed questionnaire, structured interviews were conducted with UPC leaders and nurse managers from four high-performing units to explore alignment between leadership behaviors demonstrated in practice and those identified in the literature. The qualitative data collected was thematically coded and analyzed across roles to identify the recurring themes.
Outcomes: Following the interviews, a consensus emerged regarding the leadership behaviors that contributed to the individual success of the UPCs. Relational leadership, consistent support and shared decision-making emerged as key drivers of UPC effectiveness, aligning closely with evidence from literature. UPC leaders consistently expressed that feeling supported and empowered by their nurse manager was crucial for their ability to lead. These best practices were integrated into annual NPG training to elevate and standardize UPC performance.
Recommendations: The findings from this initiative underscored the critical role of leadership behaviors in the success and sustainability of UPCs. It is recommended to integrate these best practices into leadership development programs and ongoing NPG training. Nurse managers should be equipped with tools and strategies to cultivate relational leadership, provide visible and meaningful support, and facilitate collaborative decision-making. By standardizing these leadership behaviors, organizations can strengthen the foundation of NPG, enhance nurse engagement, and improve patient outcomes. Continued evaluation and feedback from UPC leaders will be essential to refine these practices and ensure their sustained impact across the organization.
-

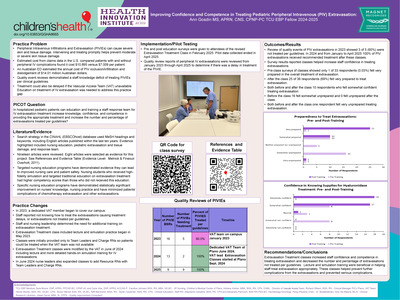
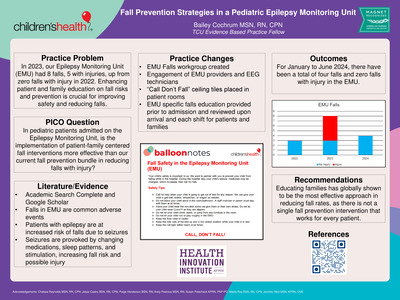
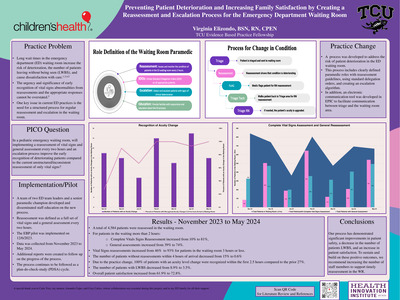
Improving Confidence and Competence in Treating Pediatric Peripheral Intravenous Extravasation
Ann Gosdin
Practice Problem: Peripheral Intravenous Infiltrations and Extravasation (PIVIE) can cause severe skin and tissue damage. Prompt intervention helps prevent moderate or severe skin tissue damage. In the U.S. PIVIE complications can cost $10,895 versus $7,009 per patient without PIVIE. An Australian ED estimated the annual cost of PIV occlusion/infiltration and dislodgement of $14.01 million Australian dollars.
Quality event reviews demonstrated a staff knowledge deficit of treating extravasations per guidelines. Treatment could be delayed if the Vascular Access Team (VAT) was not available. Education on treatment of IV extravasation was needed to address this practice gap.
PICO(T) Question: In hospitalized pediatric patients can education and training a staff response team for IV extravasation treatment increase knowledge, confidence, and competence in providing the appropriate treatment and increase the percentage of extravasations treated per guidelines?
Literature/Evidence: Search strategy in the CINAHL (EBSCOhost) database used MeSH headings and keywords, including English articles published within the last ten years. Evidence highlighted included nursing education, pediatric extravasation and tissue damage, and response team.
Targeted nursing education programs have demonstrated they can improve nursing care and patient safety. Nursing students who received high-fidelity simulation and targeted traditional education on extravasation treatment had higher competency scores than those who did not received this education.
Specific nursing education programs have demonstrated statistically significant improvement on nurses' knowledge, practice and minimized patients' complications of chemotherapy extravasation.
Practice Change(s): In 2023, a dedicated VAT member began staffing our campus. Staff reported not knowing how to treat extravasations, causing treatment delays, or extravasations not being treated per guidelines. Staff and nursing leadership determined the need for additional training on extravasation treatment.
Extravasation Treatment classes including lecture and skills practice began in May 2023. Classes were provided only to Team Leaders and Charge RNs so patients could be treated when the VAT team was not available. Classes were modified by VAT in June 2024 including lecture and hands skills training for PIVIEs. In June 2024 nurse leaders expanded classes to add Resource RNs with Team Leaders and Charge RNs.
Implementation/Pilot Testing: Pre / post education surveys were given to attendees of the revised Extravasation Treatment Class in February 2025. Pilot data collection ended in May 2025.
Quality review reports of PIVIEs were reviewed from January 2023 through April 2025 to determine if there was delayed treatment or PIVIE not treated per guidelines.
Outcomes/Results: Quality reports of PIVIEs in 2023 showed 3 of 5 (60%) were not treated per guidelines. In 2024 and from January to April 2025 100% of PIVIEs received recommended treatment after these classes.
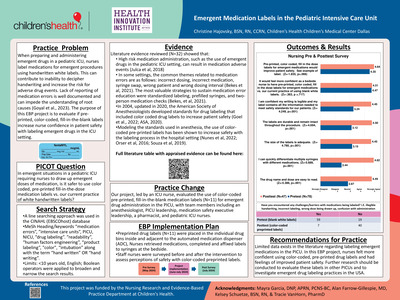
Surveys showed classes increased staff confidence in treating extravasations. In pre-class surveys classes only 1 of 33 respondents (0.03%) felt very prepared in overall treatment of extravasation. After classes 25 of 36 respondents (69%) felt very prepared to treat extravasation.
Recommendations/Conclusions: Lecture and skills training were beneficial in helping staff treat PIVIE per guidelines. Extravasation Treatment classes increased staff confidence and competence in treating extravasation and decreased the number and percentage of PIVIEs not treated per guidelines. -

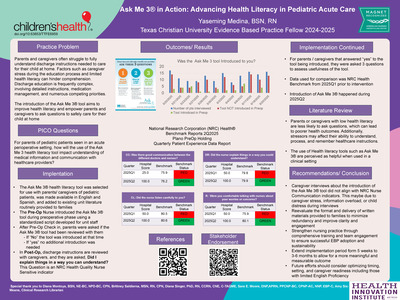
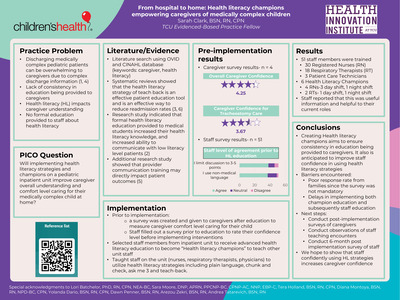
Ask Me 3® in Action Advancing Health Literacy in Pediatric Acute Care
Yaseming Medina
Background: Parents and caregivers’ understanding of how to provide safe and effective care at home is vital. However, elevated levels of stress and limited health literacy face significant challenges in understanding discharge instructions.
For parents of pediatric patients seen in an acute perioperative setting, how will the use of the Ask Me 3® health literacy tool impact understanding of medical information and communication with healthcare providers?
Literature Evidence: Patients who understand heath instructions make fewer mistakes when they take their medicine, follow treatment plans, and prepare for medical appointments (Six-Means, Amy, et al, May 2012). Patients have reported higher satisfaction and found that the use of Ask Me 3® was helpful in learning more about their medical condition (Vaillancourt & Cameron, May 2021).
Practice Changes: Multidisciplinary team lead initiative, including Unit coordinator, patient care techs, and unit nurses. Unit printed The Ask Me 3® handout in both Spanish and English and provided to caregivers during the preoperative phase. Postoperative nurses reviewed discharge instructions and Project leader assessed if the Ask Me 3® tool was reviewed with them, if they found it useful, and if they felt confident in caring for their child at home.
Implementation: The Ask Me 3® handout was introduced by nursing staff during the preoperative phase using a standardized script. Caregivers of pediatric patients were asked after preoperative check in was completed and postoperatively if the tool had been reviewed. If not reviewed, it was introduced at that time. Discharge instructions were reviewed during the post-operative phase and included Did I explain things in a way you can understand? This question is a National Research Corporation (NRC) Health® Nurse Sensitive indicator. The introduction of the Ask Me 3® tool was tracked, and NRC scores were compared across quarters using the NRC Health benchmarks from 2025 Quarter1 (2025Q1) as baseline and 2025 Quarter2 (2025Q2) post-intervention.
Results: The intervention led to marked improvements and outperformed the benchmarks set by the NRC Health® in Care Coordination, Careful listening, Patient Education, Responsiveness Communication, and Service Recovery. Caregivers who felt that communication between the different doctors and nurses improved from hospital score of 25.0 in 2025Q1 to 100.0 in 2025Q2. Similarly, caregivers reported that discharge instructions clear and surpassed the set benchmark and 2025Q1 hospital score of 50.0 to 100.0 in 2025Q2. Comfort in talking to nurses about their worries or concerns as well as their perception of the nurse listening carefully to them also outperformed the 2025Q1 hospital scores and set benchmarks from 50.0 to 100.0, respectively.
Conclusions: Ask Me 3® tool was effective in improving communication, clarity, and caregiver confidence in understanding postoperative discharge instructions. Challenges in implementation including caregivers’ recollection about the introduction of the Ask Me 3® tool when interviewed, information overload, and or child distress during interviews. Recommendations include revaluating the format and delivery of written materials to reduce redundancy, improve clarity, and caregiver engagement. Next steps include fostering team involvement, ongoing evaluation of the Ask Me 3® tool and how written materials presented to caregivers ensure long-term sustainability and adoption. -

Empowering Nurses: A Training Initiative on Essential Oils for Pediatric Neurosurgery Patients
Sheri Sacks
PICO Question: In pediatric neurosurgical bedside nurses, does education on lavender essential oil, compared to no education, improve knowledge, confidence and intent to integrateit as a complementary therapy for TBI patients?
Literature Review: Pediatric neurosurgery patients often face increased anxiety and agitation. Nurses may lack knowledge of non-pharmacological interventions to reduce agitation and anxiety in their patients. Literature review used MeSH Headings and keywords to find recent English articles. Evidence shows EO reduces anxiety. Lavender inhalation lowers anxiety, pain, and vital signs in pediatric dental patients. In adults, aromatherapy decreases anxiety, pain, blood pressure, and improves sleep, also reducing pain and extubation time.
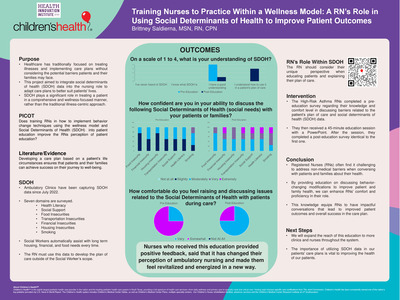
Evaluation: Nurses' knowledge of EO benefits was evaluated, and education was provided in staff meetings. Twenty-two nurses completed the pre-questionnaire and twenty-seven the post-questionnaire. In the pretest, 73% of nurses had experience using EO, compared to 59% in the posttest. EO use was mainly seasonal. Most nurses(86%) had never received EO education in the pretest, compared to 59% in the posttest. In the pretest, 87% rated their understanding of EO as slightly or not at all knowledgeable, decreasing to 71% in the posttest. Only 59% were likely or very likely to consider lavender EO for pain, agitation, or anxiety in neurosurgery patients in the pretest, compared to 92% in the posttest. Before education, 59%believed neurosurgery patients could benefit from EO, increasing to 85% after. All felt they gained some or comprehensive knowledge, and 92% wanted more EO education. EO education boosted nurses' knowledge and willingness to use EO with pediatric neurosurgery patients.
Children's Health is proud to present the posters of our EBP Fellows. Many of our nursing EBP Fellows graduate from Texas Christian University, but other universities are also attended by our graduates.
You can view them as a Collection here, or by year through our Exhibits.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.





















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}