

-

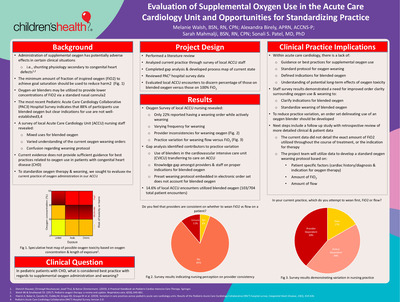
Evaluation of Supplemental Oxygen Use in the Acute Care Cardiology Unit and Opportunities for Standardizing Practice
Melanie Walsh, Alexandra Birely, Sarah Mahmalji, and Sonali S. Patel
RESEARCH
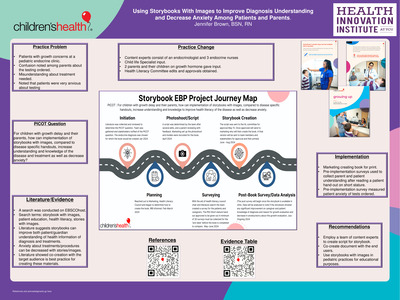
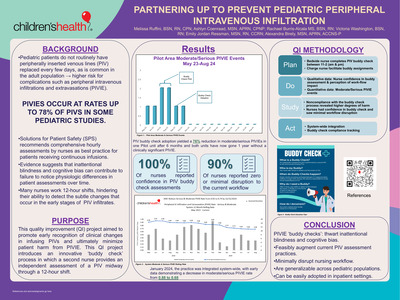
Purpose:
Oxygen delivery via nasal cannula is a standard therapy in hospitalized pediatric patients; however, it can have adverse effects in certain populations, such as infants with cardiac shunting physiology1,2. An oxygen-air blender can be used via standard nasal cannula to provide the lowest amount of fraction of inspired oxygen (FiO2) in order to reduce harm2. A recent Pediatric Acute Care Cardiology Collaborative (PAC3) Hospital Survey indicates that 88% of participating acute care cardiology units (ACCU) provide blended oxygen to patients, however, indications for use are not well-established3,4. A local ACCU nursing staff survey revealed mixed use of blended oxygen and variable understanding of current oxygen weaning orders and protocols. A literature search did not provide sufficient guidance on oxygen use best practices in patients with congenital heart disease. We sought to evaluate the current practice of oxygen administration in our ACCU.Project Design:
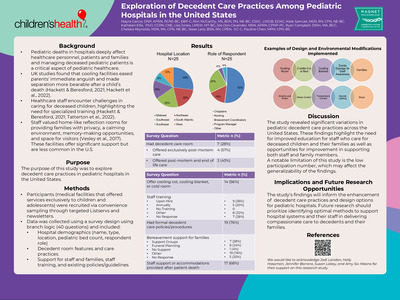
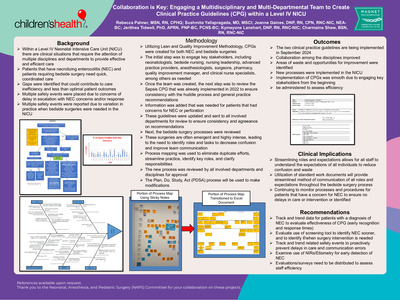
Data extraction from PAC3 registry for local ACCU encounters on oxygen use for patient encounters since October 2021. Multidisciplinary group convened to outline patient and data field inclusion criteria. Data evaluated for all ACCU encounters for patients on supplemental oxygen via nasal cannula. A gap analysis and a process map were utilized to better understand the current state.Results::
704 ACCU patient encounters used supplemental oxygen, of which 14.6% utilized blended oxygen. Analysis revealed confusion of electronic medical record (EMR) oxygen weaning led to varying approaches for choosing amount of flow versus amount of concentrated oxygen (FiO2) as the weaning mechanism. Additional causes included standard use of blenders in the cardiovascular intensive care unit, a knowledge gap of the proper indication for blended oxygen, and lack of guidelines for weaning oxygen.Conclusion:
Best practice guidelines nor standard oxygen weaning protocol exist for blended oxygen use in patients with congenital heart disease. Future steps include analysis of patient-specific factors related to the use of blended oxygen to establish best practice guidelines.References:
1. Dietrich Klauwer, Christoph Neuhaeuser, Josef Thul, & Rainer Zimmermann. (2019). A Practical Handbook on Pediatric Cardiac Intensive Care Therapy. Springer.
2. Walsh, B. K., & Smallwood, C. D. (2017). Pediatric oxygen therapy: a review and update. Respiratory care, 62(6), 645-661.
3. Hoerst, A., Bakar, A., Cassidy, S. C., Clabby, M., Grippo, E. D., Graupe, M., ... & Pediatric Acute Care Cardiology Collaborative (PAC3). (2019). Variation in care practices across pediatric acute care cardiology units: Results of the Pediatric Acute Care Cardiology Collaborative (PAC3) hospital survey. Congenital Heart Disease, 14(3), 419-426.
4. Pediatric Acute Care Cardiology Collaborative (PAC3) hospital survey, Version 3.0. -

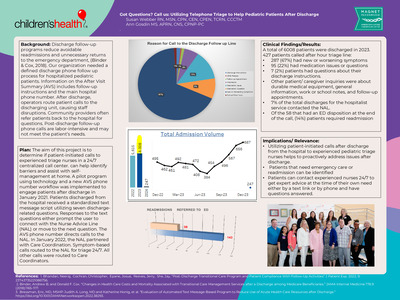
Got Questions? Call us: Utilizing Telephone Triage to Help Pediatric Patients After Discharge
Susan Webber and Ann Gosdin
EBP
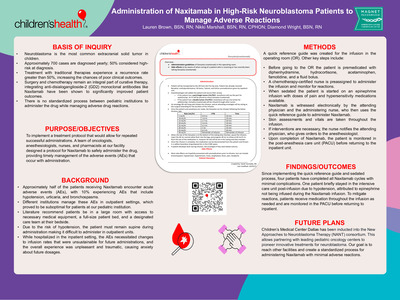
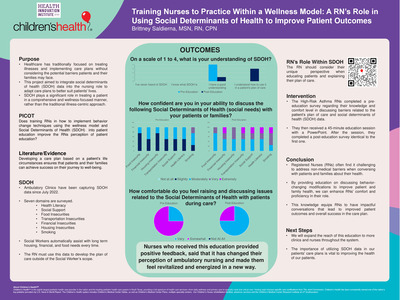
Background: Discharge follow-up programs help to reduce avoidable readmissions and unnecessary returns to the emergency department. Our organization lacked a clearly defined post-inpatient discharge process for patients on the hospitalist service. Information on the after-visit summary (AVS) includes follow-up appointment instructions and lists the main hospital phone number. Primary care providers often refer patients back to the hospital for questions related to the hospital stay. Post-discharge follow-up phone calls are labor-intensive, hard to sustain, and may not meet the patient’s needs. We sought a technology solution to assist and engage families post-discharge.
Purpose: This project aims to determine if patient-initiated calls to experienced triage nurses in a 24/7 centralized call center can identify barriers and assist with self-management at home.
Implementation: Leveraging technology and a new AVS phone number workflow, we implemented a pilot program to engage patients after discharge in January 2021. Patients discharged from the hospitalist service received a standardized text message script comprising seven discharge-related questions. In the technology solution, responses to the text questions either prompt the user to connect with the Nurse Advice Line (NAL) or move to the next question. The phone system identifies calls originating from either discharge method, and lines are open 24/7. In January 2022, the NAL partnered with Care Coordination. Symptom-based calls route to the NAL for triage 24/7, and all other call types route to the NAL after business hours.
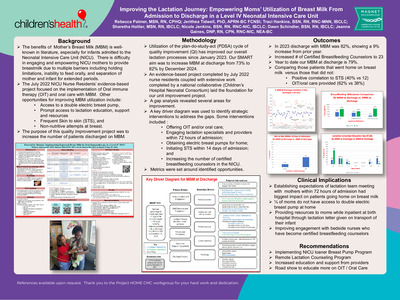
Outcomes: In 2023, the hospitalist service discharged 2,305 patients.
For Quarter 1 of 2023, the NAL managed 95 calls. Of those, 56 had new or worsening symptoms, 24 had a medication issue or questions about their medications, and three had questions about their discharge instructions. The remaining had inquiries about durable medical equipment, general information, work or school notes, and follow-up appointments.
For Quarter 2 of 2023, the NAL managed 220 calls. Of those, 144 had new or worsening symptoms, 51 had a medication issue or questions about their medications, five had questions about their discharge instructions, and the remaining DME, general information, work or school notes, and follow-up appointments.
Of the 315 patient calls for 2023, 39 patients required readmission.
Relevance: This poster will enable the learner to understand why pediatric patients call after hours and meet them at their time of need for prompt answers.
- Binder, Andrew B. and Donald F. Cox. “Changes in Health Care Costs and Mortality Associated with Transitional Care Management Services after a Discharge among Medicare Beneficiaries.” JAMA Internal Medicine 178.9 (2018):1165-1171
- Bressman, Eric, MD, MSHP: Judith A. Long, MD and Katherine Honig, et al. “Evaluation of Automated Text Message-Based Program to Reduce Use of Acute Health Care Resources after Discharge.” doi:10.1001/jamanetworkopen.2022.38293
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}