

-

Ready, Set, CODE! Investigating the Use of Two Standardized Resuscitation Algorithms to Improve Outcomes in Patients in a Level 4 NICU
Lauren Ayala, Grace Farina, Shelby Hudson, Anna Nguyen, Mireya Ortiz, and Luke Wuesthoff
EBP
Background:
Resuscitation efforts can be challenging in a Level IV NICU. Most Heath Care Providers in pediatric hospitals are Pediatric Advanced Life Support (PALS) certified. Some NICU providers are certified in both Neonatal Resuscitation Program (NRP) & PALS. There is concern regarding use of NRP vs PALS for Level IV NICU patients who are up to one year of age. Strategies need to be identified to assist nurses in determining which resuscitation algorithm (PALS or NRP) to utilize during a code/peri-arrest event involving patients in a Level IV NICU.PICO:
Will designing a resuscitation tool improve outcomes and effectiveness of code/peri-arrest events for patients in a Level IV NICU (on or off unit) in a large pediatric hospital?Literature Review:
Ten articles were reviewed relating to this topic, including literature reviews, qualitative studies, quantitative studies, & systematic reviews. Currently, there is no national guideline which suggests when it is appropriate to transition from utilizing NRP to PALS in the neonatal population. The literature suggests there is a lack of data on the outcomes of NRP vs PALS when performed on neonates. This creates confusion among staff during arrest eventsEvaluation:
Effective execution of either algorithm is better than no standardization.One code algorithm does not fit all Level 4 NICU patients. One algorithm is not better than the other. Age and etiology are important in determining best resuscitation plan for NICU patients. Further investigation of PALS and NRP are needed to determine a standardized practice since there is a lack of data to support one or the other. Practice implications are discussed. -

Optimized Pain Management Protocol for Pediatric Needlestick Procedures: Boosting Team Coordination and Pain Relief
Dhanu N. Bhandari
EBP
PICOT Question:Among clinical staff in the Integrated Therapy Unit (ITU), how does the implementation and education of a standardized set of topical anesthetic agents affect staff consistency with the new pain management procedure over six months compared to existing inconsistent practices?
Background:Effective pain management during pediatric needlestick procedures is critical but often neglected, leading to immediate distress and long-term issues like needle phobia. Research shows that proper pain management not only reduces pain but also improves patient satisfaction and clinical outcomes. However, inconsistent use of strategies like topical anesthetics has hindered optimal care. This project aimed to standardize pain management practices in the ITU to enhance patient comfort and staff efficiency, guided by evidence-based models and the Plan- Do-Study-Act (PDSA) Cycle for continuous improvement.
Literature Review:The importance of pain management during pediatric needle procedures is well-established. Evidence shows that topical anesthetics significantly reduce pain and anxiety in children. For example, Cho and Choi (2021) found that combining distraction techniques with topical anesthetics effectively reduces needle-related pain, improving outcomes. Monk et al. (2023) highlighted the success of the "Poke Plan," a structured protocol that enhanced pain management through comprehensive education and clear procedures for staff. Frameworks like the Johns Hopkins Nursing Evidence-Based Practice Model and the Iowa Model support continuous education, resource availability, and the consistent integration of evidence-based practices into care.
Evaluation:The protocol's success was assessed through pre- and post-implementation audits, focusing on the consistent use of topical anesthetics. Before implementation, only 21% of patients received adequate pain management, which increased to 67% post-implementation, marking a 46% improvement. Ongoing evaluation includes monitoring adherence, resource availability, and the effectiveness of education. Feedback from staff and patients continues to guide further improvements. The increased compliance highlights the protocol’s positive impact, with continued efforts needed to sustain and enhance these practices.
-

Management of Failure to Thrive in an Infant with Unrepaired Congenital Heart Disease: A Case Study on Energy and Nutrient Dense Formula
Alexandra Birely and Sarah Dundas
EBP
Introduction: Infants with congenital heart disease (CHD) are at risk for malnutrition and failure to thrive (FTT). Preoperative nutritional status impacts postoperative outcomes; thus nutrition should be optimized before surgery. Unrepaired infants have higher energy requirements & fluid restrictions, posing challenges in promoting growth for surgery. Energy and nutrient-dense formula has successfully treated FTT in the postoperative phase, however, evidence is limited in unrepaired infants.
Case Description: The case presented is a 4-month ex-36 week infant, past medical history significant for CHD with large ventricular septal defect (VSD), atrial septal defect (ASD), pulmonary stenosis and solitary kidney. Following discharge after birth, numerous formula changes were made due to concerns for significant weight loss, dropping below 3rd percentile by 3 weeks. Attempts to increase caloric density with hydrolyzed powdered formula resulted in persistent symptoms of vomiting, constipation and skin sensitivities. While changing to a partially hydrolyzed low lactose formula improved symptoms, weight gain couldn’t be achieved despite 27kcal/oz density. At 5 weeks patient was admitted with severe malnutrition/FTT, initiating tube feedings and reflux medication for emesis. Multiple readmissions occurred for weight concerns and feeding intolerance despite attempts to implement a suitable formula and medication regimen. At 10 weeks they initiated an energy and nutrient-dense formula which ultimately yielded rapid improvement in weight gain in subsequent weeks awaiting surgery. Prior to converting the patient gained 0.53 grams per day and the subsequent 44 days averaged 22.6 grams per day of weight gain. The patient saw improvement in constipation but retching and emesis continued.
Conclusion: Patients with left to right shunts are at risk of FTT & feeding intolerance. A severely malnourished patient demonstrated inability to increase caloric density with standard hydrolyzed formulas. Converting to low osmolality nutrient-dense formula yielded improved tolerance and weight gain, a pattern mirroring prior studies. In the setting of reduced gut perfusion, lower osmolarity formula may facilitate enhanced intestinal absorption and should be explored in a larger sample.
-

Closing the Gap for Psychiatric Resource Nurse Orientation
Kelly Bonilla, Madison McQueen, Cornelius Metili, and Annietra Udoh
EBP
A nursing orientation program can positively impact new nurses that are joining the organization (Nobles, 2022). The implementation of a new psychiatric nurse role within the hospital system developed the necessity for an orientation program that would provide quality, safe, and positive outcomes. Psychiatric Resource Nurse roles were created within the organization to provide support and education to staff regarding patients with behavioral or mental health needs. An orientation program was created to support the specific role of the Psychiatric Resource Nurse role to fulfill the need for patient centered care.
A need for an orientation program for Psychiatric Resource Nurses was evident through the lack of completion of onboarding requirements. Incomplete daily tasks, miscommunication amongst staff, inaccuracy in restraint charting, and inadequate patient care within the role needed to be addressed. The initial orientation consisted of shadow shifts, evidence based online competencies, reviewing general safety guidelines, and policies. Initial gaps were identified and utilized to formulate a new orientation program.
The new orientation framework includes three weeks of the preceptor acting as an instructor, model, and coach (Beth Tamplet Ulrich & Sigma Theta Tau International, 2019) to provide a positive orientation process. Three additional weeks established for orientee to be independent. The current Psychiatric Resource Nurse team consists of eleven Registered Nurses and one RN Team Leader. Two RNs onboarded at the time that the new orientation was implemented.
The expectations of orientation program is for the oncoming RN to be competent, confident, and comfortable in the Psychiatric Resource Nurse role by providing quality care to patients. The two RNs that completed orientation with the new orientation framework have been successfully completing Psychiatric Resource Nurse tasks for approximately 6 months. There has been improvements in completing daily tasks, restraint charting accuracy, and team collaboration. Ongoing studies show that orientation programs motivate RNs to adhere to their required duties (Lalithabai, 2021).
-

A Transformative Leadership Approach to Reducing Nursing Turnover in a Pediatric Cardiac Intensive Care Unit
Deniro Brown, Lindsey Daigle, Brandi Brown, Julia Gerstmann, Emily Hernandez, Delaney O’Brien, Casey Conrad, Christina Whittington, Lindsey Wren, and Gustavo Barbero
INNOVATION
Introduction/Objective:
Retention of nurses in the pediatric cardiac intensive care unit (CICU) is essential for optimal patient outcomes, as nurse experience significantly impacts patient mortality and hospital-acquired conditions. In April 2022, our CICU faced high voluntary turnover among direct bedside nurses. Our immediate goal was to reduce this turnover, with a longer-term objective of improving overall nurse retention.Methods:|
We established global and SMART aims by comparing organizational benchmarks for nurse turnover with unit-specific data from human resources. Co-managers and eight nurse team leaders conducted stay interviews with direct bedside nurses during the first half of 2022. These interviews revealed that key drivers for nurse retention included staff and leadership engagement, while a healthy work environment, professional development, and a positive ethical climate were secondary factors. Based on these findings, we worked with executive, physician, and human resources stakeholders to implement several interventions. These included increasing paid time off (PTO), holding listening sessions with Heart Center leadership and human resources, enhancing clinical advancement roles, involving nurses in the hiring process, and organizing monthly sessions on resilience, ethics, staff support, and engagement. These strategies were rolled out starting in the third quarter of 2022 and continued throughout 2023.Results:
In April 2022, voluntary nurse turnover in our CICU was 38.1%, the highest since the current co-managers began their roles in December 2021. The benchmark for acceptable turnover is ≤13%. By April 2023, voluntary turnover had decreased by 78%. The rolling 12-month turnover rate for 2023 was 13.1%, marking a 27.8% improvement from 2022's rate of 18.1%.Conclusion:
Targeted interventions can significantly improve nurse retention in pediatric CICUs. Enhancing engagement among nurses and leaders has proven crucial for maintaining a dedicated workforce. Despite progress, further efforts are needed to address turnover among first-year nurses. Assessing staff wellbeing with a reliable tool could provide insights to better support the workforce and further reduce turnover, fostering a resilient team and a positive workplace culture. -

The Use of Storybook Implementation for Patient Education Tools
Jennifer Brown
EBP
Practice Problem: For children with growth delay and their parents, how can implementation of storybooks with images, compared to disease specific handouts, increase understanding and knowledge of the disease and treatment as well as decrease anxiety? It was identified that parents and patients coming to the Endocrine Clinic for growth delay, did not always fully understand the reasons for the growth evaluation or causes of growth delay.
Literature/Evidence: Literature was retrieved, appraised, and synthesized to define best practices to create storybooks. Best practices included, using storybooks that include images, co-creation with intended audience. Using storybooks for patient education has been shown to have better outcomes including the ability to better understand concepts to which they may not typically be exposed, increased medical knowledge, better confidence in caring for child, increased adherence to treatment plans and decreased anxiety.
Practice Change: A team consisting of content experts worked together to co-create a storybook detailing a child’s first visit to the endocrine clinic for growth concerns. A draft was sent to two patients taking growth hormone and their parents for edits and feedback and all edits included in final draft.
Implementation: After approval from the health literacy committee, the book went to marketing for artwork and development. It has now gone to print and should be available in the next weeks to be distributed to all new patients coming for growth concerns. Pre-implementation data obtained to measure parent understanding and anxiety of the diagnosis and work up required after review of a short stature one page education sheet and visit with the physician. All children ages 7 and up are also given the survey to measure understanding and anxiety. Post-implementation data will be gathered once the book is available.
Recommendations: Clinicians should increase use of and/or create storybooks with images for patient education use.
-

Administration of Naxitamab in High-Risk Neuroblastoma Patients to Manage Adverse Reactions
Lauren Brown, Nikki Marshall, and Diamond Wright
INNOVATION
Neuroblastoma is the most common extracranial solid tumor in children with approximately 700 cases diagnosed yearly. Children treated with traditional therapies experience a recurrence rate over 50%, increasing the chances of poor clinical outcomes. Integrating anti-disialoganglioside-2 (GD2) monoclonal antibodies like Naxitimab have significantly improved patient outcomes. However, there is no standardized process between pediatric institutions to administer the drug while managing adverse drug reactions. Naxitimab received accelerated approval from the US Food and Drug Administration for children over age one with relapsed/refractory high-risk Neuroblastoma. Approximately half of the patients receiving Naxitimab encountered acute adverse events (AEs). Different institutions manage these AEs in outpatient settings, which proved to be suboptimal for patients at our facility. While hospitalized, the AEs necessitated changes to infusion rates that were unsustainable for future administrations and created a negative experience for families. Understanding the impact this monoclonal antibody has on improving clinical outcomes, our goal was to implement a treatment protocol that would allow for repeated successful administrations. Therefore, a team of physicians, nurses, and pharmacists designed a sedated protocol for Naxitimab to safely administer the drug, providing timely management of the AEs.
Prior to OR the patient is premedicated to minimize the risk of reactions. A chemotherapy-certified nurse is preassigned to administer the infusion using a QRG and monitor for reactions. When sedated, the patient is started on an epinephrine infusion with pain and hypersensitivity medications available. Skin assessments and vitals are taken throughout the infusion and if interventions are necessary, the nurse notifies the attending physician, who gives orders to the anesthesiologist. Upon completion of Naxitimab, the patient is monitored in the post-anesthesia care unit (PACU) before returning to the inpatient unit.
Initially, Naxitimab treatments faced challenges due to adverse events (AEs). However, since implementing the QRG and sedated processes, four patients have completed all cycles with minimal complications.
-

Fall Prevention Strategies in a Pediatric Epilepsy Monitoring Unit
Bailey Cochrum
EBP
Practice Problem: In 2023, our Epilepsy Monitoring Unit (EMU) had 8 falls, 5 with injuries, up from zero falls with injury in 2022. Enhancing patient and family education on fall risks and prevention is crucial for improving safety and reducing falls.
Literature: Falls in an EMU are common adverse events. Patients with epilepsy are at increased risk of falls due to seizures. In the EMU, seizures are provoked by changing medications, sleep patterns, and stimulation, increasing fall risk and possible injury.
Practice Change(s): For planned EMU admissions, we developed additional seizure-specific education for patients and families, sent prior to admission and reviewed upon arrival and each shift. We also added "Call Don't Fall" signage and ceiling tiles in patient rooms.
Implementation/Pilot Testing: We developed a workgroup compiled of bedside nurses, a clinical nurse specialist, advanced practice provider, and unit leadership to research falls in other EMUs to see what practices we could incorporate to keep our patients safe. The practice changes were implemented beginning in December 2023.
Outcomes: For January to July 2024, we had four total falls and zero falls with injury in our EMU.
Recommendations/Conclusions: It is our hope that families are prepared for their EMU admission. Families need to know what to expect when admitted into our EMU and to work with us to keep their child safe. Educating families has globally shown to be the most effective approach in reducing fall rates, as there is not a single fall prevention intervention that works for every patient.
-

BRIDGING THE GAP: LEVERAGING CNAP TO ENHANCE PROFESSIONAL DEVELOPMENT, ALIGN WITH ORGANIZATION GOALS AND CREATE A CULTURE OF SAFETY
Marissa Crosley, Brooke Harris, Gwenetta Hicks, and Cornelius Metili
INNOVATION
Abstract: As our organization strives for its fifth Magnet designation, enhancing nurse professional development has become a clear priority. Currently, only half of our nursing staff participate in the Clinical Nurse Achievement Program (CNAP), highlighting a need for increased engagement. Additionally, feedback from the latest Experience, Inclusion, and Engagement (EIE) Survey identified an opportunity to improve nurse recognition within our department. These insights prompted an exploration of how the Team Lead role, uniquely positioned between frontline nurses and leadership, could be more effectively utilized.
A key challenge identified is the time-consuming process of documenting CNAP achievements. Nurses often defer this task until just before the deadline, leading to rushed, less reflective, and sometimes incomplete submissions. This perceived burden reduces engagement and undermines the program's effectiveness, aligning with broader findings that Clinical Ladder Programs (CLPs), though beneficial, are often seen as onerous due to extensive documentation requirements (Meucci, Moore, & McGrath, 2019). Additionally, the lack of visibility around CNAP success stories further decreases motivation among nurses to participate.
Recent studies, including research by the American Organization for Nursing Leadership (AONL) (Grenny, Begley, & Hancock, 2023), emphasize the importance of leadership in fostering professional growth and recognition. Genuine leadership engagement—demonstrating care, facilitating growth, and providing help—has been shown to promote a positive and supportive work environment. In response to these insights, our department strategically leveraged the CNAP as a vehicle for more meaningful engagement, revising the image of the nurse leader as a catalyst for professional development. This presentation will discuss how, with structured support—including participation in team lead forums, Magnet Ambassador participation, regular 1:1 managerial mentorship, improved submission processes, and increased visibility of CNAP achievements—our department achieved a 25% increase in certified nurses and a 50% increase in CNAP participation, reinforcing our commitment to excellence and supporting the advancement of our Magnet journey.
References:
Grenny, J., Begley, J., & Hancock, A. (2023). Leadership's role in fostering professional growth and recognition: Findings from the American Organization for Nursing Leadership and Crucial Learning. American Organization for Nursing Leadership.
Meucci, J. M., Moore, K., & McGrath, A. (2019). The complexities of documenting professional activities in Clinical Ladder Programs. Journal of Nursing Administration, 49(11), 561-568.
Meucci, J., Moore, A., & McGrath, J. M. (2019). Testing evidence-based strategies for clinical ladder program refinement. Journal of Nursing Administration, 49(11), 561-566.
Grenny, J., Begley, R., & Hancock, B. (2023). Connection is retention: The power of care, growth, and help in nurse leadership. Crucial Learning and the American Organization for Nursing Leadership.
-

From Identification to Action: Nurses Respond to Human Trafficking
Misty Daugherty, Jill Hanks, Alison Kell, Annie Tolliver, Katie Fields, and Lily Velez
INNOVATION
Background: In 2022, nurses from a pediatric healthcare system hosted a Human Trafficking Conference to educate healthcare providers on the identification of human trafficking victims. In post-conference surveys, participants reported a gap in their ability to respond once a human trafficking victim was identified. The conference planning committee reconvened in 2023 to address this gap and shifted from a didactic presentation to application and simulation.
Purpose: Research shows in our home state, there are about 313,000 people being trafficked, up to 50% of them being youth. It is estimated that up to 88% of human trafficking victims encounter healthcare providers while being trafficked. The majority of healthcare providers report feeling ill-equipped to identify the warning signs and lack training in trauma-informed care. There is a need to address this gap in training with opportunities for healthcare workers to apply their knowledge in a low-stakes environment.
Implementation: The 2023 conference offered survivor testimonies and an expert panelist. The planning committee designed breakout rooms featuring standardized patient scenarios, simulation utilizing the Greenbaum Screening tool, activation of healthcare system protocols, and an escape room. The content was strengthened by partnering with content experts from the healthcare system, community trafficking organizations, and local and federal law enforcement agencies. These experts were able to share real-life experiences in supporting victims of human trafficking.
Evaluation: The 2023 post-conference survey demonstrated successful closure of the application gap for participants, with 100% of the 68 respondents stating that they felt “comfortable initiating the next steps in escalation once a potential trafficked victim is identified.” Remarkably, 95.6% of respondents indicated feeling “comfortable using a trauma-informed approach”.
Recomendations: Children who are victims of human trafficking are coming into our workplaces. Pediatric nurses must learn their role in identifying victims, providing trauma-informed care, how to report, and what policies and guidelines are in place. We must advocate for the training to provide care for this vulnerable population.
References:
/="/">1.) Combs, M. A. (2021). Human trafficking: Empowering healthcare providers and community partners as advocates for victims. Journal of Holistic Nursing, 40(3), 302-303. DOI: 10.1177/08980101221116444
/="/">2.) Dols, J. D., Beckmann-Mendez, D., McDow, J., Walker, K., & Moon, M. D. (2019). Human trafficking victim identification, assessment, and intervention strategies in South Texas emergency departments. Journal of emergency nursing, 45(6), 622-633.
/="/">3.) Exeni McAmis, N.E., Mirabella, A.C, McCarthy, E.M., Cama, C.A., Fogarasi, M.C., Thomas, L.A., Feinn, R.S. ; Rivera-Godreau, I. (2022). Assessing healthcare provider knowledge of human trafficking. PloS ONE, 17(3),e0264388. DOI: 10.1371/journal.pone.0264338
/="/">4.) González-de la Torre, H., Hernández-De Luis, M.-N., MiesPadilla, S., Camacho-Bejarano, R., Verdú- Soriano, J., Rodríguez-Suárez, C.-A. (2024). Effectiveness of “escape room” educational technology in nurses’ education: A systematic review. Nursing Reports, 14(2), 1193–1211. https://doi.org/10.3390/ nursrep14020091
/="/">5.) Lorvinsky, J., Pringle, J., Filion, F., Gagnon, A. J. (2023). Sex trafficking survivors’ experiences with healthcare system during exploitation: a qualitative study. PloS One, 18(8), e0290067. DOI: 10.1371/journal.pone.0290067
/="/">6.) Miller, C. L., Chisolm-Straker, M., Duke, G., & Stoklosa, H. (2020). A framework for the development of healthcare provider education programs on human trafficking part three: recommendations. Journal of human trafficking, 6(4), 425-434.
/="/">7.) Ortman, K, Sullivan, K. Hansen, K. (2021). Barriers to addressing human trafficking in healthcare. South Dakota Medicine: The Journal of the South Dakota State Medical Association, 74(12), 584-585. -

Improving Sepsis Response, Awareness, and Engagement in the Emergency Department
Virginia Elizondo, Nicole Bizzack, Amber Dayton, Angie Rodick, Ashley Collins, Georgina Hernandez, and Amber Albiar
QUALITY
Sepsis background:
Sepsis is the leading cause of death in children2 and a global health problem3. The primary source of infection is often not apparent1, making early patient identification, initiation of sepsis protocols, and continued awareness crucial to improve outcomes and prevent mortality in patients at risk for sepsis.Purpose:
An emergency department (ED) Sepsis Response Team (SRT) and other initiatives were designed to enhance workflow efficiency, improve time to antibiotic administration (TTA) tominutes, improve sepsis recognition, and uphold standards by maintaining staff engagement.Implementations:
Once a patient screens positive for sepsis risk, an SRT is immediately activated. A multidisciplinary team responds and promptly initiates treatment in accordance with sepsis protocols. In contrast, patients identified as high-risk upon arrival were directly taken to a room where the interdisciplinary team met them. Treatments were administered according to standing delegation orders and an algorithm for accessing ports/PIVs. Ongoing education, coaching, and skills development were prioritized to enhance sepsis recognition. An Escape Room simulation was also created to promote staff engagement and reinforce the importance of following sepsis protocols.Results:
Over twenty-seven months, data tracked improvements in TTA. The percentage of patients utilizing a SRT increased from 42% to 58% in April-December 2022, rose to 76% in 2023, and reached 81% in June 2024. The high-risk population TTA increased from 59% to 85% in April-December 2022, reached 97% in December 2023, and remained 97% in May 2024. Sepsis recognition improved from 75% in 2023 to 88% in 2024 through the proper utilization of the screening tool. Staff engagement was evident in the Escape Room participation, with 100% of the participants successfully escaping within 12-14 minutes.Conclusion:
Implementing new processes, education, and engagement initiatives through a collaborative approach has dramatically improved TTA and transformed the sepsis culture in the ED. The data shows that a multi-faceted approach involving the nursing staff and valuing everyone's contribution is crucial for improving sepsis care quality.References
Hilarius, K. W., Skippen, P. W., & Kissoon, N. (2020). Early recognition and emergency treatment of sepsis and septic shock in children. Pediatric Emergency Care, 36(2), 101–106. https://doi.org/10.1097/pec.0000000000002043Lane, R. D., Richardson, T., Scott, H. F., Paul, R. M., Balamuth, F., Eisenberg, M. A., Riggs, R., Huskins, W., Horvat, C. M., Keeney, G. E., Hueschen, L. A., Lockwood, J. M., Gunnala, V., McKee, B. P., Patankar, N., Pinto, V., Sebring, A. M., Sharron, M. P., Treseler, J.,...Workman, J. K. (2024). Delays to antibiotics in the emergency department and risk of mortality in children with sepsis. JAMA Network Open, 7(6), e2413955. https://doi.org/10.1001/jamanetworkopen.2024.13955
Martínez, M., Plata-Menchaca, E. P., Ruiz-Rodríguez, J., & Ferrer, R. (2020). An approach to antibiotic treatment in patients with sepsis. Journal of Thoracic Disease, 12(3), 1007–1021. https://doi.org/10.21037/jtd.2020.01.47
-

Preventing Patient Deterioration by Creating a Reassessment and Escalation Process for the ED Waiting Room
Virginia Elizondo, Amanda Caipo, and Cory Carlos
EBP
Practice Problem:
Long wait times in the emergency department (ED) waiting room significantly impact patient outcomes. Waiting times increase the risk of deterioration, the number of patients leaving without being seen (LWBS), and lead to dissatisfaction with care. 1,2,3 The urgency and significance of early recognition of abnormal vital signs and the appropriate responses cannot be overstated.3 Current ED practices lack a structured process for regular reassessment and escalation in the waiting room.
Literature/Evidence:
A comprehensive literature search was conducted, utilizing EBSCOhost, PubMed, and Ovid. The literature supports continuous reassessment to enhance safety and satisfaction in the waiting room.
Practice Change:
The new initiative aimed to improve the early recognition of deteriorating patients in the ED waiting room. This group developed a process that defined waiting room staff roles with reassessment guidelines, standard delegation orders, and the implementation of an escalation algorithm. In addition, an electronic communication tool was created.
Result:
Seven months of data were collected. Significant improvement was noticed in the frequency of reassessment. Full set of vital signs for patients waiting more than 2 hours rose from 10% to 81%. General assessments increased from 39% to 74%. Reassessments of vital signs at 3 hours or less from arrival to the waiting room rose from 46% to 93%. In contrast, the number of patients in the waiting room for more than 4 hours without a reassessment decreased from 15% to 0.6%. Of the patients with an acuity level change, 100% were recognized within the first 2.5 hours compared to the prior 27%. The percentage of patients LWBS decreased from 8.9% to 3.5%. The overall patient satisfaction increased from 61.9% to 72.8% during the pilot.
Conclusions:
The new process has demonstrated significant improvements in patient safety, a decrease in the number of patients LWBS, and increased patient satisfaction. This initiative cultivates cooperative work and proactive interventions between nurses and paramedics that enhance patient care and safety.
References
Burgess, L., Kynoch, K., & Hines, S. (2019). Implementing best practice into the emergency department triage process. International Journal of Evidence-Based Healthcare, 17(1), 27–35. https://doi.org/10.1097/xeb.0000000000000144
/="/">Innes, K., Jackson, D., Plummer, V., & Elliott, D. (2021). Exploration and model development for emergency department waiting room nurse role: Synthesis of a three-phase sequential mixed methods study. International Emergency Nursing, 59, 101075. https://doi.org/10.1016/j.ienj.2021.101075
/="/">Spechbach, H., Rochat, J., Gaspoz, J.-M., Lovis, C., & Ehrler, F. (2019). Patients' time perception in the waiting room of an ambulatory emergency unit: A cross-sectional study. BMC Emergency Medicine, 19(1). https://doi.org/10.1186/s12873-019-0254-1 -

Exploration of Central Venous Catheter Protective Devices in the Pediatric Population: A Mixed Methods Study
Lindsey Flores, Quineka Smith, Maria Leal, and Melissa Ruffini
RESEARCH
Purpose:
/="/">In the pediatric population, about 25% of the catheters are reported to have issues such as CLABSI, line dislodgement, contamination, or catheter breaks. The primary purpose of this study is to explore caregiver and nurse satisfaction of pediatric patients with CVCs that utilize a wearable protective device with specific aims to determine parent’s perception of the feasibility while wearing the device. Wearable devices are an extra measure utilized among pediatric patients for nurses and parents to further protect the CVC dressing and catheter from complications. A single site study found that utilizing a wearable device reduced line trauma and infections.Methods:
/="/">Utilizing a mixed method cross sectional design in the setting of a large pediatric hospital located in the South, we used 2 different samples. The samples included parents with children that have CVCs and nurses caring for children with CVCs. These 2 groups were purposively sampled for feasibility through interviews and satisfaction surveys. The parents were provided education during the consent process. Feasibility interviews took place in person or via phone at 1-3 weeks post study enrollment. Satisfaction surveys were emailed to parents at 30-day intervals for 3 months. Nurses caring for patients while using the device were asked to complete a satisfaction survey via QR code or emailed link.Results:
/="/">There is limited literature on interventions to maintain children’s optimal activity levels without compromising the securement of CVC. This study added to the existing literature by exploring the parents’ viewpoint on the feasibility of using this device along with parents’ and nurses’ satisfaction. Qualitative analysis revealed two major themes. THEME 1: “Physical Details of Gus Gear: Positive Experiences and Benefits” THEME 2: “Challenges and Recommendations”. Quantitative analysis to be completed at the end of Feb 2025. -

Exploration of Decedent Care Practices Among Pediatric Hospitals in the United States
Mayra Garcia, Kim McCarthy, Kiele Samuel, Kathleen Ellis, Lisa Jones, Joe Don Cavender, Ryan Campbell, Chelsea Reynolds, Jesse Leos, and Pauline Chen
RESEARCH
Purpose:
Pediatric deaths in hospitals profoundly affect both staff and families, underscoring the need for clear decedent care processes and specialized training to navigate emotional and procedural challenges. Cooling rooms and reflection spaces, which provide families with more time for memory-making and help ease the emotional burden of separation, have been shown to offer significant support. However, these facilities are less common in the U.S., highlighting the necessity for further research in this area. The purpose of this study was to explore the decedent care (DC) practices in pediatric hospitals in the United States.Methods:
Participants were recruited via forwarded emails and Listservs utilizing a survey design. Survey data collected including demographic details such as hospital name, type, location, pediatric bed count, and the role of the survey respondent. Additional data on decedent room features, family and DC practices, staff and family support, staff training, and existing policies or guidelines was also collected.Results:
This study surveyed pediatric hospitals (N=25) to assess the availability and use of decedent rooms. The findings revealed that 28% of these hospitals had decedent rooms. Of these, 57% exclusively offered post-mortem care, while 43% also provided end-of-life care. Decedent care (DC) was multidisciplinary, encompassing support for both staff and families. Various design and environmental modifications were implemented across hospitals. Staff training and its frequency varied by hospital (72%), as did the resources and support available to staff. Formal policies and procedures for decedent care were established in 76% of hospitals.Discussion:
The study revealed significant variations in pediatric decedent care practices across the United States. These findings highlight the need for improved education for staff who care for deceased children and their families.Implications:
The study's findings will inform the enhancement of decedent care practices and design options for pediatric hospitals. Future research should prioritize identifying optimal methods to support hospital systems and their staff in delivering compassionate care to decedents and their families. -

Emergent Medication Labels in the Pediatric Intensive Care Unit
Christine Hajovsky
EBP
PICOT: In emergent situations in a pediatric ICU requiring nurses to draw up emergent doses of medication, is it safer to use color coded, pre-printed fill-in-the-dose medication labels vs. our current practice of white handwritten labels? In our pediatric ICUs, nurses use handwritten labels for emergent drug administration, which can lead to illegibility and increased risks of adverse events. This project assessed whether pre-printed, color-coded, fill-in-the-blank labels enhance nurse confidence and nurses’ perceptions of patient safety during emergent drug procedures.
Literature/Evidence: Search strategy in the CINAHL (EBSCOhost) database used MeSH headings and keywords, including English articles published within the last ten years. Evidence highlighted that adopting color-coded labels, modeled after anesthesia standards, can improve drug labeling safety in hospitals.
Evaluation: Led by an ICU nurse, our project implemented color-coded, pre-printed labels in a PICU. Our team included an anesthesiologist, PICU leadership, pharmacists, and ICU nurses. New drug labels were placed in individual drug bins inside and adjacent to the medication dispenser, where nurses retrieved medications, completed and affixed labels to syringes at the bedside. Staff nurses were surveyed before and after the intervention to assess their perceptions of safety with color-coded preprinted labels. Surveys conducted pre and post intervention indicated significant improvements in nurses' ability to differentiate syringes (25% to 96%) and confidence in label legibility and completeness (51% to 91%). Overall confidence in using color-coded labels for emergent procedures improved (87% to 96%). Initially, 82% of nurses agreed that these labels would enhance patient safety, which rose to 96% post-intervention. While literature on PICU medication labeling is limited, our project demonstrated that color-coded, pre-printed labels bolster nurse confidence and perceived patient safety. Further research is warranted to validate these findings across diverse PICU settings.
-

Development of ECLS Transport Checklist
Laura Hatton, Lakshmi Raman, Donna Taylor, and Margarita Ramos
QUALITY
Purpose: To develop a tool that will prevent complications related to transporting patients on ECLS thereby improving positive outcomes.
Background: In 2021, a patient on ECLS was transported from the unit to acquire imaging. The usual practice was to obtain an X-ray to confirm cannula placement after a transport. However, the X-ray was not obtained when the patient got back to the unit and unbeknownst to the team, the patient’s cannula had significantly moved despite visualization of intact sutures. The change in cannula position was not discovered until the morning X-ray that was taken several hours later. When the X-ray plate was taken out from under the patient, the cannula became dislodged.
Methodology: It was determined that a tool was needed to ensure that all safety steps during and after an ECLS transport are completed. A transport checklist was created that consists of three parts: 1. Safety checklist prior to departure for transport; 2. Designated responsibilities/roles of staff; 3. Checklist upon arrival that includes an X-ray confirming cannula and ETT placement. The checklist requires the ECMO attending to sign off on it that the above were completed.
Results: Since the institution of the ECLS Transport Checklist, there have been 52 off unit transports of ECLS patients with no complications or injuries related to ECLS transport.
Conclusion: The ECLS Transport Checklist has improved closed loop communication and has effectively prevented the omission of integral safety measures when transporting an ECLS patient.
-

Residency Resources to the Rescue!
Jill Hesler and Martha Shaw
INNOVATION
Collaboration and communication between residency facilitators and residency coordinators is imperative to overall nurse residency program and individual resident success. Increased cohort sizes and the lasting impact of a global pandemic to academia continued to contribute to a noticeable trend in nurse residents’ failure to progress. Failure to progress is defined as an inability to move forward during unit level orientation. Signs of failure to progress may include inability to perform new tasks or tasks previously completed, lack of interest in new opportunities, and anxiety disproportionate to the situation. This upward trend was made evident by an increase in requests for transfer to a different clinical area due to lack of confidence or concern for the resident’s ability to be successful, frequent use of the Residency Rescue Guidelines, and an increase in orientation action plans (OAPs). This provided more opportunities for facilitators and coordinators to work together to support resident success.
/="/">Residency Rescue Guidelines provide an algorithm with opportunities and support available to nurse residents in collaboration with residency coordinators, unit leadership, and human resources. OAPs are education support documents outlining SMART goals specific to hurdles the nurse resident is facing, preventing orientation progression. Along with OAPs, an Individualized Learning Plan (ILP) was implemented to proactively provide support to residents struggling during orientation. Implemented during the early phase of the residency rescue algorithm, an ILP allows coordinators to collaborate with the resident, residency facilitator, and unit leadership to develop a plan tailored to meet the learning needs of the resident. The use of the Residency Rescue Guidelines, OAPs, and ILPs together prompts timely communication for residents who are at risk for failure to progress. ILPs and OAP are being leveraged for around 5% of residency cohorts, resulting in residents successfully completing orientation and being retained to the organization. -

Little Lungs, Big Care: Prevent Unplanned Extubation
Leslie Huntington, Emily Jordan Ressman, and Carmen Yearego
QUALITY
Background: The pediatric critical care unit in a large medical center benchmarks a variety of quality metrics to ensure we are providing our patients with the best care. At the end of 2023, the unit rate of 0.58 was higher than the national benchmark rate of 0.33 for unplanned extubation (UE). Additionally, the unit was lower for failed extubation rate than the national benchmark which led to questioning if the unit was too conservative with when patients are deemed ready to extubate.
Objectives: The primary goal is to lower the rate of UE while maintaining a failed extubation rate lower than the national benchmark. The secondary goal is to reduce the time between extubation readiness testing (ERT) or a spontaneous breathing trial (SBT) and extubation.
Methods: A quality improvement (QI) team was created and tasked with an urgent timeline to reduce UE. The team implemented a peri-extubation checklist and has completed three PDSA cycles in the first 6 months of the project. Data collection began in April and will complete in August 2024.
Results: The 2024 UE rate through June decreased 87% when compared to the 2023 rate through June. With the average UE costing $101,0001, this is a reduction in costs of $707,000 through Q2 2024. The baseline time elapsed between an ERT/SBT and extubation was a median of 11.5 hours during Q4 2023. Utilization of the checklist decreased that time to a median of 6 hours and 34 minutes. This is a statistically significant reduction with p < 0.01. The year-to-date failed extubation rate was 2.79% as of June 2024. This is largely unchanged from 2023. Staff feedback was also generally positive.
Conclusion & Implications: Short-term QI projects such as checklist development can encourage multidisciplinary engagement and reduce the frequency of unplanned events.
1Solutions for Patient Safety (2017). SPS Value Calculator. [Excel file]. Retrieved from www.solutionsforpatientsafety
-

Exploring Parent/Child Peri-Anesthesia Anxiety and Anesthesia Effects on Children
Ann Johnson, Alejandra Lozano, and Pauline Chen
RESEARCH
Approximately four million children undergo procedures with anesthesia yearly. For children and parents, this can be anxiety-provoking. In extant literature, level and timing of pre-anesthesia anxiety in children are not adequately studied; associated factors are largely unknown in humans. Preparing for anesthesia and its effects may cause parental worry, and little is known about these effects on school-age children in the weeks following a procedure. The purpose of this study was to explore longitudinal peri-anesthesia factors of anxiety and behavior in children ages 7 through 12. Spanish and English-speaking dyads consented to four data collection points beginning at the pre-anesthesia clinic (visit #1) when the Zero to Ten visual analog scale for child anxiety and the adult State Anxiety scale were administered. The child scale was repeated on procedure day (visit #2). The Post Hospitalization Behavior Scale for Ambulatory Surgery was administered to parents two and four weeks after anesthesia. Using Wilcoxon signed-rank test, parametric, and nonparametric analysis, results of the first 66 dyads reveal children have significantly higher (2nd quartile) anxiety on visit #2 compared to visit #1 (p< .001), with a weak correlation to parent anxiety at both visits. Spanish-speaking parents feel significantly less prepared for their child’s anesthesia (p< .001) and have significantly higher pre-anesthesia state anxiety levels vs. English-speaking parents (p< .005). Child post-anesthesia behavior scores are in the first quartile (mild), decline over time, and are not significantly related to anesthesia duration. In conclusion, pre-anesthesia anxiety exists in 7 to 12-year-olds, particularly on the day of their procedure. Parental anxiety has little effect on child pre-anesthesia anxiety, however, lack of knowledge and higher state anxiety in the Spanish-speaking parent subset is concerning. Anesthesia duration has no significant effect on post-anesthesia behavior. In the future it is important to assess and address child anxiety, parent knowledge, and to reassure parents regarding mild post-anesthesia behavior difficulties that typically resolve.
-

NICU Team Nursing Model: Purposeful Collaborative for Positive Outcomes
Kymeyone Lanehart, Rebecca Palmer, Jerithea Tidwell, Lisa Mason, Sharica Whitten, Katie Doerge, and Sushmita Yallapragada
INNOVATION
Background: In 2013, an elevated CLABSI rate as high as 3.4 indicated that a specialized team approach would be necessary to improve quality care and patient outcomes. Development of a unique blood stream infection (BSI) team, that focused specifically on managing central lines, was successful and later expanded in to focus on other quality metrics. In 2015, the team was re-named safety and quality (SAQ). In 2016, the NICU utilized the team model by developing an internal transport team (ITT) to complete internal transports for procedures. The SAQ and ITT groups merged in 2019 to improve efficiency in the unit workflow and to promote team development. Currently, known as the transport and quality team (TAQ), there is continued evolution, where the team has extended their skills to respond and treat moderate and severe peripheral intravenous infiltrates (PIVIEs) with Wydase administration, insertion of midline catheter devices and peripherally inserted central catheters (PICCs).
Objective: Implement team-based nursing model to ensure patient safety and improve quality measures of the neonate on a variety of platforms which include appropriate vascular access, peripheral and central line management, internal transport and prevention of hospital acquired conditions (HACs).
Implementation:
- Role Development and team member selection process
- Competency pathways (initial and ongoing)
- Team Interventions and bundles: CLABSI, PIVI, CAUTI, HAPI
- Internal Transport Standards
- Line management and insertion guidelines
- Escalation and communication processes
- Shift reports and data collection
Evaluation:
- Increased bundle compliance >90%
- Increased vigilance of reporting and reviewing (Safelinks, Escalation, Audits)
- Increased professional practice (certifications)
- Departmental collaboration (MRI, IR, Fluoroscopy, Nuclear Medicine, Radiology)
- Improved clinical team communication
- Decreased HAC events/rates
- Improved line management
- Decreased central line days 0.28%
- Improved department workflow
- Gallup: Improved staff engagement and satisfaction
-

Midline Catheter Implementation: Expanding Vascular Access Options in a Level IV NICU to Decrease Vascular Injury
Kymeyone Lanehart, Rebecca Palmer, Jeri Tidwell, Sushmita Yallapragada, Courtney Campbell, Lebanon David, and Katie Doerge
EBP
Background: PIV catheters are the most placed device in the NICU requiring frequent attempts, with a brief duration due to complications which indicate removal before completion of treatment. PIVs used for treatment have a patient safety risk of PIVIE; the severity can be mild, moderate, or severe depending on the swelling and tissue damage. PIVIE rates are one of the patient quality outcomes and are increasing in the NICU. Considering the increased risks of long-term consequences from tissue injury associated with PIVs, MCD may improve quality and patient outcomes.
Problem: PICOT question: (P)For eligible neonates in a level IV NICU, (I) will implementation of midline catheters, (C) compared to the use of non-midline PIVs, (O) reduce the incidence of serious PIVIEs, (T) six months after full implementation.
Conceptual Framework:
Iowa Model Revised: Evidence-Based Practice to Promote Excellence in Health CareLiterature Review
- Midline catheters are longer than standard PIVs and offer longer dwell times.
- Common placement of midline catheters is for difficult access.
- Use methods to select the appropriate vascular access device for patient’s needs.
- Validates standard PIVs are the most placed device in the NICU yet have a risk for complications and patient harm.
- Regarding effectiveness in reducing vascular injuries in NICU patients, midline catheters need further reported data.
Methodology
- Revise NICU Appropriate Line Algorithm to include midline catheters.
- Product trial Benchmarking
- Create guidelines for use of midline catheters
- Develop education for staff.
- Utilize specialized team for line insertion and management.
- Data collection of PIVIEs and midline performance
Data Analysis
Analyze and compare number of PIVIEs in the NICU 6 month pre- and post-implementation.Interpretation
Midlines have longer dwell times, less complications, and decreased PIVIE events. -

Ironing Out the Details: Early Detection and Treatment of Iron Deficiency in a Level 4 NICU
Rachel Mills
EBP
Practice Problem: In a level 4 neonatal intensive care unit (NICU), no standardized method existed for identifying and treating iron deficiency (ID) in preterm or low birth weight (LBW) infants. Common practice was to adjust iron supplementation based on hematocrit levels, though this was not based on any formal protocol or guideline. ID of the brain in neonates may be associated with neurologic and developmental deficits. Thus, it is prudent to identify and treat early. In a recent survey, providers reported a lack of familiarity with biomarkers for early identification of ID.
Literature/Evidence: A comprehensive review of the literature utilizing PubMed was completed. This revealed that traditional hematological methods of monitoring for ID, such as hematocrit, may be poor indicators of brain iron status. Reticulocyte hemoglobin (Ret-He) is supported in the literature as a highly valuable method for early detection of ID in neonates. Recent benchmarking data revealed that approximately 40% of surveyed NICUs are using Ret-He to identify ID and about half have a standardized protocol for monitoring and treating ID.
Practice Change: Based on the evidence, an algorithm was created to provide guidelines for monitoring and treating ID using Ret-He levels. Education regarding use of the algorithm was provided to physicians, advanced practice providers, bedside nurses and dietitians.
Implementation/Pilot Testing: Routine ordering of Ret-He for eligible patients was trialed for 7 weeks, and the proposed algorithm was followed.
Outcomes/ Results: 32 patients met inclusion criteria during the pilot period. Ret-He orders were placed for 94% (30) of these patients. There were 6 occurrences of low Ret-He with hematocrit >30%, indicating early detection of ID. Iron supplementation was adjusted per the algorithm.
Recommendations/Conclusions: Review of published work, benchmarking data and pilot testing support the use of a standardized guideline with routine checking of Ret-He as best practice for identification and treatment of ID in preterm and LBW infants.
-

Nurse Manager Hiring Practices and the Experience of New Graduate Nurses
Tiffany Montgomery and Zara Sajwani-Merchant
RESEARCH
Purpose
/="/">Hiring decisions have implications for the hiring unit and the healthcare organization, including nursing retention, orientation costs, and organizational culture. Despite available literature, hiring practices, and diversity, equity, and inclusion practices are unknown within nurse residency programs. This study explores the experiences of nursing hiring managers and newly hired nurse candidates with the interview and hiring process into residency programs within the DFW metroplex.
/="/">Methods
/="/">A qualitative phenomenological study was conducted to describe the nursing manager experiences and thoughts through the hiring process and how they compare to nurse candidate’s perspective hired into an established nurse residency program. Purposive sampling identified eligible study participants using the DFW Hospital Council.
/="/">Semi-structured, virtual interviews with hiring managers and newly hired nurse candidates were conducted to gain a better understanding of the hiring process. An interview guide with open ended questions, along with probing questions to encourage the participant to elaborate on the details to achieve clarity and stay close to the lived experience, guided the interviews. Sampling continued until thematic saturation with no new themes emerging in the interviews.
/="/">Transcripts from nurse candidates and nurse managers were documented on the word document. Each transcript was read multiple times by at least two members of the research team. Key ideas and codes were identified from each transcript. Mutual consensus on codes was periodically conducted to ensure all members of the research team agreed on the identified codes. Similar codes were grouped into broader themes.
/="/">Results
/="/">Two themes developed from the data of nurse candidates. Theme 1 was “Process of Hiring” and theme 2 was “Experiences, Assumptions, and Biases”. The first theme “Process of Hiring” entails two categories (I) “Organization and Specialty-Based Differences” and “Interview Format and Structure”. Theme 2 emerged from nurse candidate interviews “Experiences, Assumptions, and Biases” entails two categories, “Program Tenure and Overall Experience” and “Perceptions of Receiving Job Offer” mentions views of nurse candidates on factors influencing getting a job offer including educational organizations, clinical experience, work history, passion for working, etc.
/="/">Two themes developed from the data of nurse managers. Theme 1 was “Hiring Process and Role of Manager” and theme 2 was “Hiring Biases and Ways to Reduce it”. The first theme “Hiring Process and Role of Manager” entails two categories “Screening and Selection” and “Interview Structure and Format.” Theme two “Hiring Biases and Ways to Reduce it” caters to three categories: “Factors Impacting Hiring, ” “Source of Bias,” and “Strategies to Limit Bias.” -
 - Transformational Leadership Strategies that Create the Foundation for EBP Enculturation by Sara Moore, Kathleen Ellis, Zara Sajwani-Merchant, and Lindsey Patton")
Owning your Practice through Evidence-Based Practice (EBP) - Transformational Leadership Strategies that Create the Foundation for EBP Enculturation
Sara Moore, Kathleen Ellis, Zara Sajwani-Merchant, and Lindsey Patton
INNOVATION
Background: Nursing Research and Evidence-Based Practice (NREBP) is central to advancing nursing science and integrating nursing practices supported by scientific inquiry to improve health outcomes and quality of care1,4. The gap between what nurses know and what they do can have life-altering consequences2,7 . The degree to which nurses base their practice behaviors on research, EBP competence, and use of EBP skills is sub-optimal and is directly influenced by organizational and institutional barriers3. Common barriers to implementing EPB behavior change include organizational culture, leadership, networks and communication, resources, evaluation, monitoring and feedback, and availability of qualified EBP mentors5. Supportive work environments and proactive leaders are necessary to create cultures conducive to EBP. To mitigate the barriers to EBP and build EBP capacity, the NREBP program developed strategy, resources, and professional development opportunities for clinical nurses and leaders.
Implementation: Creating the infrastructure to support clinical nurses by providing resources, including EBP experts, is essential. The NREBP team is developing an EBP infrastructure by creating frameworks, processes, certification supports, professional development opportunities, and interprofessional collaborations. The NREBP team is developing engagement through rounding with clinical nurses to understand resource needs, implementing and further studying the EBP Leadership Behavior Program, developing pathways to support EBP mentors through further skill development and facilitation, and EBP professional development plans for all Children’s Health nurses. This year, our team has onboarded 350 nurse residents, increased the pool of EBP mentors, submitted an EBP study to the IRB, initiated an EBP competency building rubric, supported nursing/unit/organization/DNP EBP projects, supported 13 EBP fellowship projects, and initiated an EBP mentorship program.
Evaluation: Since 2020, this work has resulted in a 263.6% increase in nurses participating in EBP, 140% in EBP nurse fellows, 88% increase in abstracts submitted to conferences, and 84% increase in the number of publications. Strategic planning and leadership development to enculturate EBP raises the organizational capacity to transform EBP.
1. Chien, Li-Yin. (2019). Evidence-based practice and nursing research. The Journal of Nursing Research, 27(4), e29.
2. Dakka, F.J. (2022). Nurses barriers to evidence-based practice in palliative care: A systematic review. SAGE Open Nursing, 8, 1-8. https://Doi.org/ 10.1177/23779608221142957
3. Laibhen-Parks, N., Kimble, L., Melnyk, B., Sudia, T., & Codone, S. (2018). An adaptation of the original FRESO test to measure evidence-based practice competence in pediatric bedside nurse, Worldviews on Evidence-Based Nursing, 15(3), 230-240.4. Lal, M. (2021). Why nursing research matters. The Journal of Nursing Administration, 51(5), 235-236. doi: 10.1097/NNA.0000000000001005.
Why Nursing Research Matters - PubMed (nih.gov)
5. Li, H., Tyson, S., Meyers, E. A., Ada, H., & Jordan, M. (2023). Advancing EBP culture and competencies through an academic‐research partnership: Process and outcomes of an EBP scholar program. Worldviews on Evidence-Based Nursing, 20(1), 44-46. https://doi.org/10.1111/wvn.12616
6. Speroni, K., Mclaughlin, M., & Friesen, M.A. (2020). Use of evidence-based practice models and research findings in magnet-designated hospitals across the United States: National survey results. Worldviews on Evidence-Based Nursing, 17(2), 98-107.
7. Wentland, B. A., & Hinderer, K. A. (2020). A nursing research and evidence-based practice fellowship program in a magnet®-designated pediatric medical center. Applied Nursing Research, 55, 151287-151287. https://doi.org/10.1016/j.apnr.2020.151287 -

Mindful Cleanliness: Resetting Expectations for Environmental and Personal Hygiene to Reduce the CLABSI Rate in a Level IV NICU
Rebecca Palmer, Kymeyone Lanehart, Jerithea Tidwell, Sushmita Yallapragada, Jeanne Gaines, and Courtney Campbell
QUALITY
Background
/="/">CLABSIs place patients at high risk for mortality and morbidity, increasing length of stay, and additional costly and detrimental therapeutic interventions. Our NICU historically had a better than national average CLABSI rate, however, since 2022, our CLABSI rate spiked to above average. During this timeframe the unit experience higher census and acuity leading to increased workload and needs of patients and staff. In 2022, the CLABSI rate spiked from 0.53 in 2021 to 1.04 and 1.12 CLABSIs/1000 line days in 2022 and 2023, respectively.Methodology
/="/">Utilizing Quality Improvement methodology allowed identification of the root cause of the increase in CLABSIs within our unit. After each CLABSI, a bedside review was completed identifying cause of infection. After evaluating trends, the majority of CLABSIs were due to skin or GI bacteria, highlighting a decrease in the unit’s environmental and personal hygiene practices. SMART Aim: Decrease CLABSI rate to < 0.9 CLABSIs/1000 line days by December 2024. To improve overall cleanliness and awareness within the unit, interventions put into place included:- “Days Since” in multidisciplinary daily huddle
- Transition to Five Moments of Hand Hygiene
- Availability of hand sanitizer on bedside carts
- Disposable curtain trial
- Midline implementation, decreasing central line days
- Bare Below the Elbows (BBE) and Wash, Wipe, Wear (3Ws) – nothing below the elbow, improved environmental hygiene, and effective hand washing
Outcomes
/="/">After implementation of interventions identified, intentional auditing, and Just In Time Training, hand hygiene compliance increased to >95% consistently for all moments of hand hygiene. Identifying gaps and barriers in cleanliness allowed interventions to be implemented and PDSA cycles allowed for improvement in compliance. The NICU went 230 days CLABSI free starting November 2023. Currently for 2024, the rate is 0.46 CLABSIs/1000 line days. -

A Methodical and Multidisciplinary Approach to Reducing Unplanned Extubationin a Level IV NICU
Rebecca Palmer, Ashley Reed, Reed Graham, Nimrod Otieno, Veronica Contreras, Jeanne Gaines, Jerithea Tidwell, Alice Figueroa, Travis Reynolds, Syed Ahmed, and Sushmita Yallapragada
QUALITY
Background: Unplanned extubations (UE) in neonates can result in severe consequences such as airway obstruction, hypoxia, respiratory distress, and even death. It is crucial to prevent UEs to maintain stable breathing, minimize the need for reintubation, and improve outcomes for neonates in the neonatal intensive care unit (NICU). The multidisciplinary NICU UE team has been working to prevent UEs since 2017. After an increase in 2022, the team conducted an evaluation to identify potential gaps and discovered over 50% of patients were not being reintubated post-event. Identified factors that contributed to UE events were: infants with weight < 4 kilograms; unadjusted high endotracheal tubes (ETT) per x-ray; inadequate sedation; lack of extubation readiness trial; and inadequate taping of the ETT. In 2022, our UE rate spiked to 0.50 UEs/100 vent days which prompted our multidisciplinary team to reinvigorate our work.
Methodology: A multidisciplinary team of NICU stakeholders implemented several interventions addressing the causal buckets of our UEs in 2022. ETT x-ray annotations, candy cane taping on neobars, and auditing of ETT securement were implemented. After reviewing causal buckets for 2023, airway cards were updated to identify high-risk patients; sedation concerns were escalated; implemented taping for patients over 4 kilograms; posted clamp-down event signage to prevent premature pulling of an ETT. Created x-ray provider escalation algorithm to promote immediate adjustment of mispositioned ETT. In 2023, the team implemented a standardized post-event response apparent cause analysis (ACA) huddle. Bedside reviews were held 7-10 days post event. Key process improvements and lessons learned were discussed and disseminated.
Outcomes: From January to June 2023, our UE rate was 0.62 UEs/100 vent days which was reduced to 0.25 UEs/100 vent days from July to December. 2023 year end rate was 0.48 UEs/100 vent days. By April 2024, our UE rate was 0.28 UEs/100 vent days. An evidence-based, multi-disciplinary approach contributed to the reduction of UEs in the NICU. Next steps are discussed.
-

Improving the Lactation Journey: Empowering Moms’ Utilization of Breast Milk From Admission to Discharge in a Level IV Neonatal Intensive Care Unit
Rebecca Palmer, Jerithea Tidwell, Traci Hankins, Sharetha Hollier, Nicole Jenkins, Dawn Schindler, and Jeanne Gaines
INNOVATION
Background
The benefits of MBM is well-known in literature, especially for infants admitted to the NICU. There is difficulty in engaging and empowering NICU mothers due to multiple barriers including holding limitations, inability to feed orally, and separation of mother and infant for extended periods. Opportunities for improving MBM utilization throughout admission include oral immune therapy (OIT) and/or oral care with MBM, skin to skin (STS), and non-nutritive attempts at breast. Access to lactation education, support, and resources throughout admission is imperative.Methodology
Utilization of the plan-do-study-act (PDSA) cycle of quality improvement (QI) has improved our overall lactation processes since January 2023.- SMART aim: Increase MBM at discharge from 73% to 82% by December 2024.
A literature review and benchmarking were completed in collaboration with the Children’s Hospital Neonatal Consortium (CHNC). Comparing best practice to current practice, it was identified the biggest opportunities included:
- OIT and/or oral care • Lactation Team engagement within 72 hours of all admissions
- Double Electric Breast Pump access
- Provider team engagement and education within 72 hours of admission
- STS within 14 days of admission
Outcomes
MBM at discharge increased from 72% in 2022 to 82% in 2023. In 2024 through July, MBM at discharge is 79%. Comparing patients that go home with MBM versus those that do not, higher rates of the following are seen:- STS (40% compared to 12%)
- Access to double electric breast pump within 72 hours (91% compared to 64%)
- OIT / Oral Care (62% compared to 38%)
When lactation team is fully staffed and available to provide education and support within 72 hours, the percent of patients discharging home with MBM is higher. There are still multiple barriers to achieve sustainability, including:
- Provider engagement
- Rate of OIT / Oral Care.
- Consistent availability of lactation support< br />
Continued work includes engagement of bedside nurses that are Certified Breastfeeding Counselors, standardized education, and pump access at home.
-
 within a Level IV NICU by Rebecca Palmer, Sushmita Yallapragada, Jeanne Gaines, Jerithea Tidwell, Kymeyone Lanehart, and Charmaine Shaw")
Collaboration is Key: Engaging a Multidisciplinary and Multi-Departmental Team to Create Clinical Practice Guidelines (CPG) within a Level IV NICU
Rebecca Palmer, Sushmita Yallapragada, Jeanne Gaines, Jerithea Tidwell, Kymeyone Lanehart, and Charmaine Shaw
INNOVATION
Background
Within a Level IV collaboration between different disciplines and departments is needed to provide care delivery that is effective and efficient. Emergent situations arise that require care to be provided quickly, including patients with necrotizing enterocolitis (NEC) and/or require bedside surgery. Upon review, multiple inconsistencies and inefficiencies were identified in these processes.Implementation
Utilizing Lean and Quality Improvement methodology, CPGs were created for both necrotizing enterocolitis and bedside surgery. The steps taken in creation of these CPG include:
• Identification of key stakeholders of all departments, including neonatology, surgery, and anesthesia
• Evaluation of the Sepsis CPG to allow for consistency in huddle practices and recommendations
• Add care specific to NEC and/or perforation based on literature review
• Once NEC CPG were finalized, bedside surgery CPG was started
• First step was to identify current state through a swimlane process map, including all disciplines and departments in the creation
• Identify areas of waste, gaps, and recommendations for new process
• Re-create swimlane process map with recommendations, and create a standard work document for all disciplines
• Include standard work documents in the bedside surgery CPG
• After creation of CPG, dissemination to all disciplines and departments to review, edit, and agree upon recommendationsEvaluation
Both CPGs went live in August 2024. Including all key stakeholders in the beginning allowed for an efficient and effective way to evaluate all care practices and recommendations moving forward. This allowed for communication about expectations for roles and responsibilities, evaluate and decrease waste, and reset expectations for all involved. Next steps will be to monitor and track consistency and utilize PDSA methodology to make modifications as needed. -
 Research Participant Consents by Beena Pappen, Lindsay Therrian, and Bobby Lawrence")
Reducing the Burden of Tracking Age of Majority (AOM) Research Participant Consents
Beena Pappen, Lindsay Therrian, and Bobby Lawrence
QUALITY
Background
/="/">Reconsenting research participants when they reach Age of Majority (AOM) – age 18 in the state of Texas – is a vital responsibility of the pediatric research world. It requires tracking and planning for an activity that may not happen until months, years, or over a decade later. Not obtaining AOM consent may violate the rights of the research participant, as well as impede the ongoing collection and usage of their research data. At the Center for Cancer and Blood Disorders (CCBD) Clinical Research Office (CRO), a very manual process was being used to identify and notify staff of upcoming AOM activities. Thus, we sought to automate the process for ease and efficiency in tracking and communicating AOM dates.Methodology
/="/">First, we transferred existing AOM tracking data from an Excel spreadsheet to a SharePoint list. Next, we determined the desired frequency, email content, and individuals to be notified of the upcoming AOM dates. Finally, we leveraged our organization’s Information Systems (IS) team to build SharePoint flows using PowerApps that enabled automated notifications and secure access.Outcomes
/="/"> The SharePoint AOM List has simplified the process for adding new participants, maintaining a current list, assigning individuals to receive notifications, and alerting staff of upcoming AOM dates. The automated emails are sent only to the assigned parties when a research participant’s AOM date is approaching within the next 30 days, 2 weeks, or 1 week.The automated method for tracking upcoming AOM dates has proven to alleviate the burden on coordinators by eliminating the need to regularly check a database for upcoming AOM dates and reducing the manual email reminders to clinic staff. With flexibility built into the design of the SharePoint list and automated flows, we can confidently track AOM participants and ensure relevant parties receive reminders in a timely manner.
-

PARTNERING UP TO PREVENT PEDIATRIC PERIPHERAL INTRAVENOUS INFILTRATION
Melissa Ruffini, Ashlyn Coenraad, Rachael Burris-Alcala, Victoria Washington, Emily Jordan Ressman, and Alexandra Birely
QUALITY
Background: Peripheral Intravenous Infiltrations and Extravasations (PIVIE) occur in up to 78% of peripheral IVs (PIVs) in some pediatric studies. Proper site assessment is essential in preventing patient harm from PIVIEs, with hourly nursing assessments considered best practice for patients receiving continuous infusions. Many nurses work 12-hour shifts, and evidence suggests that inattentional blindness and cognitive bias can contribute to failure to notice physiologic differences in patient assessments over time. To address this challenge and ensure early identification of symptoms, the local project team proposed an innovative ‘buddy check’ approach to minimize patient harm.
Methods: This quality improvement project was developed as a change idea from the larger institutional PIVIE Steering Committee, in collaboration with a nurse residency evidence-based practice project. The buddy check process was initially outlined by project leaders to include intentionally timed PIV site assessments by a second nurse, midway through a 12-hour shift. This model was piloted for feasibility on four inpatient units using plan-do-study-act (PDSA) cycles.
Results: Qualitative data from nurses demonstrated 100% confidence in peer buddy check assessments, with 90% reporting zero or minimal disruption to the current workflow. During the pilot 77 PIVIEs occurred, with a majority detected in the mild stage (71%). 55% of mild were identified during buddy checks. For PIVIEs detected at later stages, moderate to serious harm, 77% were noncompliant with buddy checks. In September 2023, one unit formally implemented the buddy check practice, yielding a 76% reduction in moderate/serious PIVIEs from the pre-implementation phase. In January 2024, the practice was integrated system-wide, with early data demonstrating a decrease in moderate/serious PIVIE rate from 0.92 to 0.80.
Conclusion: Noncompliance with buddy checks correlated with higher degrees of harm, indicating that buddy checks facilitate earlier identification of infiltration. The buddy check process is a feasible intervention to augment current practice, yielding minimal nursing workflow disruption. This intervention is generalizable and can be easily adopted across pediatric care settings.
-

New Approach to Professional Governance in Ambulatory
Brittney Saldierna, Katelyn Tinkey, and Diana Sarmiento
INNOVATION
Shared Governance Committees have involved frontline staff in driving change for many years. However, they often involve significant input from leaders, making frontline staff feel like their opinions don't matter as much. Professional Governance Committees emphasize that frontline staff should be the primary drivers of change without significant influence from leaders. Leaders should focus on removing barriers to the frontline staff's vision and ensuring that all changes comply with policies and regulations.This Ambulatory System has created a unique structure in which the Ambulatory Council (AC) is the overarching structure for nine other councils. These councils meet monthly and practice with a professional governance approach. Each council is composed of a chair, chair-elect, and three or more clinical staff members. They also have a leader sponsor at the meetings to help remove barriers and support, but not to drive the meetings. The increase in engagement is related to the impact that our frontline staff is now seeing in this “extra” work that they are doing
The AC meeting occurs quarterly with chairs, chair-elects, and ambulatory leaders. During these meetings, chairs from each council present their current project, any barriers, and ask for feedback when needed. Leaders are able to be present so that any barrier that hasn’t already been removed is well-heard and likely can be reviewed and discussed. This is a time for collaboration and feedback before a process changes begin
After our recent Magnet Survey, the AC was excited to be recognized as a best practice at our facility. Our projects and achievements are positively impacting the daily work of our staff, patient satisfaction, and patient safety. Staff members are more independent, engaged, and energized, which is contagious. It's inspiring to see their enthusiasm for their work renewed, creating a more vibrant environment. All council members and leaders are eager to see the next projects.
-

Caring for Manes: Creating Diverse Hair Care Guidelines for a Large Pediatric Hospital
Jeri Tidwell, Tiffany Montgomery, Phyllis Carter-Riles, Victoria Washington, Kym Lanehart, and Jesse Leos
QUALITY
Background
Hair care products should be available to all patients regardless of hair type and texture. Recent movements like the Crown Project sparked pediatric hospitals across the country to focus efforts on ensuring hair care equity for their patients. Children’s health joined the movement by sanctioning a multidisciplinary, multidepartment task force to address BIPOC hair concerns. A smaller group was tasked with aligning practices and policies to address the gaps in education and resources available to assist nurses in caring for ethnic hair.Methodology
Review of literature was conducted. Limited published work was found. The workgroup benchmarked and consulted with other subject matter experts and pediatric hospital leaders that completed the journey. The subgroup also reviewed relevant policies and guidelines, collaborated and with supply chain to secure safe hair care products and assisted with developing a comprehensive educationOutcomes
• A Diverse hair care guideline was developed including instruction on assessment, hair care management and use of appropriate products.
• A Comprehensive Education program was designed including hair care champions videos and hands-on practice
• A pilot is being planned for later this year.
• Practice Implications next steps will be discussed. -

CEASE the Alarms: A Nurse-Led Bundled Approach to Alarm Management
Annie Tolliver
EBP
Practice Problem:The use of audible alarms to monitor pediatric patients is crucial to patient care. Alarms notify nurses of potentially life-threatening situations. However, increasing non-actionable alarms can cause desensitization. This leads to ignoring and mismanaging alarms, ultimately putting patients at serious risk. For those caring for the sickest pediatric patients, strategies for reducing non-actionable alarms to mitigate alarm fatigue are needed to enhance patient safety.
Literature/Evidence:A review of the literature highlighted emerging evidence-based practice supporting the use of the CEASE bundle for nurse-led alarm management, as outlined in a quasi-experimental research study. Multiple systematic reviews substantiate the effectiveness of the interventions within the CEASE bundle.
Practice Change(s):CEASE is an acronym for Communication, Electrodes (daily changes), Appropriateness (evaluation), Setup alarm parameters (patient customization), and Education (initial and ongoing). These strategies work together to reduce the level of non-actionable alarms.
Implementation/Pilot Testing:A pilot of the CEASE Bundle was conducted in a pediatric intensive care unit (PICU). Pre-pilot survey data was collected on alarm management practices and perceived alarm fatigue. The PICU staff received educational sessions on alarm management and the CEASE bundle, followed by a 5-day pilot period during which nurses implemented the bundle. Alarm data was collected before, during, and after the pilot, and survey data was gathered from participating PICU nurses after the pilot.
Outcomes/Results:During the pilot period, there was a 44.17% reduction in physiological alarms on the unit compared to pre-pilot data. The pre/post survey results did not show a decrease in perceived alarm fatigue from participants but did show a decrease in the perceived frequency of non-actionable alarms and in complaints from patients/families about the level of alarms.
Recommendations/Conclusions:During this pilot period, the CEASE bundle effectively reduced the number of alarms in the PICU. Further study is recommended to understand the impact on staff's perceived alarm fatigue.
References:
/="/"> 1) Bach, T. A., Berglund, L.-M., & Turk, E. (2018). Managing alarm systems for quality and safety in the hospital setting. BMJ Open Quality, 7(3). DOI: 10.1136/bmjoq-2017-000202
/="/"> 2) Bi, J., Yin, X., Li, H., Gao, R., Zhang, Q., Zhong, T., … Li, Z. (2020). Effects of monitor alarm management training on nurses’ alarm fatigue: A randomised controlled trial. Journal of Clinical Nursing, 29(21–22), 4203–4216. DOI: 10.1111/jocn.15452
/="/"> 3) Bonafide, C. P., Localio, A. R., Holmes, J. H., Nadkarni, V. M., Stemler, S., MacMurchy, M., … Keren, R. (2017). Video Analysis of Factors Associated With Response Time to Physiologic Monitor Alarms in a Children’s Hospital. JAMA Pediatrics, 171(6), 524–531. DOI: 10.1001/jamapediatrics.2016.5123
/="/"> 4) Bosma, S., & Christopher, R. (2023). Implementing a Unit-Based Alarm Management Bundle for Critical Care Nurses. Critical Care Nurse, 43(2), 36–45. DOI: 10.4037/ccn2023418
/="/"> 5) Dee, S. A., Tucciarone, J., Plotkin, G., & Mallilo, C. (2022). Determining the Impact of an Alarm Management Program on Alarm Fatigue among ICU and Telemetry RNs: An Evidence Based Research Project. SAGE Open Nursing, 8. DOI: 10.1177/23779608221098713
/="/"> 6) Engel, J. R., Lindsay, M., O'Brien, S., Granger, C. B., Moore, E. S., Hughes, T., … Fuchs, M. A. (2022). Health System Redesign of Cardiac Monitoring Oversight to Optimize Alarm Management, Safety, and Staff Engagement. The Journal of Nursing Administration, 52(10), 511–518. DOI: 10.1097/NNA.0000000000001192
/="/"> 7) Gül, G., & İntepeler, Ş. S. (2021). Ensuring Specificity as a Strategy for Increasing Alarm Safety. Journal of Basic and Clinical Health Sciences, 7(3), 139-147.
/="/"> 8) Lewandowska, K., Weisbrot, M., Cieloszyk, A., Mędrzycka-Dąbrowska, W., Krupa, S., & Ozga, D. (2020). Impact of Alarm Fatigue on the Work of Nurses in an Intensive Care Environment-A Systematic Review. International Journal of Environmental Research and Public Health, 17(22), 8409. DOI: 10.3390/ijerph17228409
/="/"> 9) Lewis, C. L., & Oster, C. A. (2019). Research Outcomes of Implementing CEASE: An Innovative, Nurse-Driven, Evidence-Based, Patient-Customized Monitoring Bundle to Decrease Alarm Fatigue in the Intensive Care Unit/Step-down Unit. Dimensions of Critical Care Nursing, 38(3), 160–173. DOI: 10.1097/DCC.0000000000000357
/="/"> 10) López‐Espuela, F., Rodríguez‐Martin, B., Lavado García, J., Toribio‐Felipe, R., Amarilla‐Donoso, F. J., Rodríguez Almagro, J. J., … Moran‐García, J. M. (2022). Experiences and mediating factors in nurses' responses to electronic device alarms: A phenomenological study. Journal of Nursing Management, 30(5), 1303–1316. DOI: 10.1111/jonm.13614
/="/"> 11) Nyarko, B. A., Nie, H., Yin, Z., Chai, X., & Yue, L. (2023). The effect of educational interventions in managing nurses' alarm fatigue: An integrative review. Journal of clinical nursing, 32(13-14), 2985-2997. DOI: 10.1111/jocn.16479
/="/"> 12) Ruppel, H., Pohl, E., Rodriguez-Paras, C., Froh, E., Perry, K., McNamara, M., … Bonafide, C. P. (2023). Clinician Perspectives on Specifications for Metrics to Inform Pediatric Alarm Management. Biomedical Instrumentation & Technology, 57(1), 18–25.
/="/"> 13) Shaoru, C., Hui, Z., Su, W., Ruxin, J., Huiyi, Z., Hongmei, Z., & Hongyan, Z. (2023). Determinants of Medical Equipment Alarm Fatigue in Practicing Nurses: A Systematic Review. SAGE Open Nursing, 9. DOI: 10.1177/23779608231207227
/="/"> 14) Stoltzfus, K. B., Bhakta, M., Shankweiler, C., Mount, R. R., & Gibson, C. (2019). Appropriate utilisation of cardiac telemetry monitoring: a quality improvement project. BMJ Open Quality, 8(2), e000560. DOI: 10.1136/bmjoq-2018-000560
/="/"> 15) Zadvinskis, I. M., Schweitzer, K., Murry, T., & Wood, T. (2018). Tele Talks: Nurse‐Led Discussions Regarding Need and Duration of Cardiac Telemetry May Impact Alarm Fatigue, Empower Nurses, and Reduce Cost. Worldviews on Evidence-Based Nursing, 15(4), 323–325. DOI: 10.1111/wvn.12294 -

Rise of the New Grad: Early Engagement of New Graduate Nurses in Professional Governance
Annie Tolliver and Katie Fields
INNOVATION
Background: Traditionally, new graduate nurses (GNs) are advised to gain experience before participating in Nursing Professional Governance (NPG). NPG is a structure that empowers nurses to be decision-makers regarding the nursing practice environment. We identified GNs had minimal knowledge of and engagement in NPG. An innovative process was developed to involve GNs in NPG, challenging the traditional approach.
Literature: Substantial evidence supports that nurses engaged in NPG are empowered to make decisions, leading to better patient outcomes and increased professional satisfaction. Research shows GNs’ dedication and professional satisfaction are tied to their ability to embed into the organizational culture and find meaning in their work. NPG provides the opportunity to contribute meaningfully and exercise autonomy, authority, and accountability.
Implementation: In the past, nurse leaders suggested GNs focus on just “becoming a nurse” the first year. In collaboration with key stakeholders (including GNs, operational and program nurse leaders) a new vision was created. GNs now nominate and vote for their peers to become voting members representing the voice and decision-making authority of their cohort. They’re accountable for sharing information, gathering feedback, and engaging all GNs.
Evaluation: In 2022, no GNs were engaged in NPG core councils. As of Fall 2024, five GN cohorts completed this process and two have graduated residency. Now, approximately 10% of NPG Core Council membership is made up of GNs with many choosing to run for departmental membership positions upon graduating. The 2023 residency cohort has a retention rate of over 95% and 100% for those who were part of NPG.
Implications: In the evolving healthcare landscape, pediatric nurses must be actively involved in making decisions that will influence the future of nursing. NPG empowers nurses to be decision-makers, advancing nursing practice, quality, competency, and knowledge. Instead of sticking to traditional thinking that new nurses should only focus on developing their bedside skills, imagine a future where those newest to the profession are the ones improving it.
References:
1) Bartmess, M. P., Myers, C. R., & Thomas, S. P. (2022). ‘It Would Be Nice to Think We Could Have a Voice’: Exploring RN Involvement in Hospital Staffing Policymaking. AJN The American Journal of Nursing, 122(10), 22-31.
2) Clemmons-Brown, C. A. (2023). Innovation and evidence-based Decision-Making: Addressing new Graduate nurse turnover. Nursing Administration Quarterly, 47(1), E1-E11.
3) Porter-O'Grady, T., Hancock, B., & Start, R. E. (2024). Advancing Professional Governance to Improve Health Outcomes. JONA: The Journal of Nursing Administration, 54(7/8), 387-389.
4) Song, Y., & Kim, J. A. (2023). New Graduate Nurses' Competencies, Organizational Socialization, and Turnover Intention. JONA: The Journal of Nursing Administration, 53(12), 675-682.
5) Tyndall, D. E., Scott, E. S., Jones, L. R., & Cook, K. J. (2019). Changing new graduate nurse profiles and retention recommendations for nurse leaders. JONA: The Journal of Nursing Administration, 49(2), 93-98. -

High reliability pediatric heart centers: Always working toward getting better
Andrea Torzone and Alexandra Birely
QUALITY
Background
As provision of care reaches a new complexity in pediatric cardiology, programs are called upon to evaluate how they can bring their teams into the future of pediatric cardiac care. High reliability principles support high-quality care and improve outcomes, thus should be embraced to guide continuous improvement. Although much has been written about high reliability in healthcare, it has not been explored within pediatric heart centers. The purpose of this review is to examine high reliability through the lens of a contemporary pediatric heart center, elaborating on key concepts and proposed considerations for maintaining a high reliability heart center.Methodology
Core principles of high reliability were reviewed: preoccupation with failure, sensitivity to operations, reluctance to simplify, deference to expertise, and commitment to resilience. Recently published recommendations for comprehensive pediatric heart centers were evaluated and categorized, aligning with high reliability principles. Analysis identified additional drivers of high performance that were further explored in the literature. Suggestions for practical application were outlined.Outcomes
Operationalizing high reliability within a heart center can facilitate prevention of harm and optimize outcomes. Practical application of high reliability requires a shared mental model and aligns teams. Review of literature identified a gap specific to pediatric cardiology and the application of high reliability principles. Thus, we synthesized literature on relevant themes which emerged as suggested facilitators of high reliability within heart center teams. Drivers included interprofessional collaboration, recognition of nursing expertise, psychological safety, and structural empowerment void of hierarchy. Three primary conclusions were derived from this analysis. First, acknowledging culture as the underpinning of all structure and processes allows teams to rebound from failure and supports the mission of rising to exceptional patient challenges. Second, interprofessional collaboration and a flattened hierarchy support a psychologically safe environment, which in turn supports innovation. Third, but of utmost significance, innovative strategies are necessary to retain experienced pediatric nurses, which are essential for high quality patient care across the heart center. -
 Rounds with Morbidity and Mortality Review by Andrea Torzone, Glenda Moate, Linn Groom, Mary Hart, Erin Hunter-McPhan, Christa Conley, Kimberly Moore, Sarah Zoretic, Priya Bhaskar, Nicholas Andersen, Ryan Butts, and Yousef Arar")
Timeliness of “Red Event” Reviews: Optimizing “Cardiac-Multidisciplinary Assessment of Performance” (C-MAP) Rounds with Morbidity and Mortality Review
Andrea Torzone, Glenda Moate, Linn Groom, Mary Hart, Erin Hunter-McPhan, Christa Conley, Kimberly Moore, Sarah Zoretic, Priya Bhaskar, Nicholas Andersen, Ryan Butts, and Yousef Arar
QUALITY
Background:
/="/">Review of Morbidity and Mortality (M&M) events within Heart Centers (HC) is critical for improving patient care. Timely review is important to maintain transparency and accuracy in recall and produce actionable items to reduce the likelihood for similar occurrences. Cardiac-Multidisciplinary Assessment of Performance (C-MAP) rounds and M&M Selection Committee were initiated July 2020 to review surgical patient outcomes, team performance, and events deviating from expected course. M&M selection committee consists of physicians, advanced practice nurses, and quality improvement consultants to determine patients appropriate for review at M&M conference. We aim to analyze timeliness of review following patient events related to institution of C-MAP rounds and M&M selection committee.Methods:
/="/">C-MAP rounds scores patient courses based on outcomes: “on-target” (green) or deviation from the ideal with no significant lasting harm (yellow) or significant harm (red) and team performance: outstanding (4), expected (3), suboptimal (2), or poor (1). C-MAP Rounds occur within 10 days of procedure and frequently provide initial identification of events which require deeper review. Analysis of C-MAP “red ” events was performed between 2022-2023 to identify total patients reviewed at M&M selection committee. No formal procedure coordinating C-MAP and M&M committee existed. Further analysis was performed to elicit timeliness of review between event date and committee review date and was compared to timeliness prior to the initiation of C-MAP and M&M committees.Outcomes:
/="/"> “Red” events between 2022 - present were reviewed at M&M committee at a rate of 83.2% (79/95). Prior to C-MAP/M&M committee initiation, all significant patient events were reviewed on average 60.5 days (median 52 days) from event. After establishing C-MAP/M&M committee, cases were reviewed on average within 29 days (median 26 days). Instituting C-MAP rounds and M&M committees improved timely review of patient events. We now formally refer C-MAP “red” events to M&M selection committee to ensure appropriate oversight and communication of recommendations. -

Standardization of Adult Transition Across Ambulatory
Virginia Vecchio and Monica Fuller
QUALITY
Background:
Historically, at Children’s Health initiatives involving patient transition to adult care have been focused on the clinics which are ranked in U.S. News & World Report’s Best Children’s Hospitals. Other clinics had no process for transition and were unaware of available resources.
Purpose:
A subgroup from the Ambulatory Clinical Practice Council identified the need for a standardized framework and EPIC documentation that every clinic could utilize.
Methodology:
The Office of Patient Transition (OPT) was onboard with revamping the current program and allowing nurses to drive the changes. A knowledge assessment was performed with nurses in 2022. The results proved that nursing was unaware of currently resources, did not know where to document transition, and had no uniform way to transition. The subgroup of nurses then collaborated with OPT to develop a quality improvement process standardizing patient transition.
This teamwork included modifying the computer based training (CBT) modules which are taken by the entire outpatient staff, including medical staff, upon hire. Modifying a letter which is given to the patient at the beginning of their transition journey, developing a customizable process framework to be used across the ambulatory system, and creating standardized EPIC documentation are among the many modification which have been developed or are in the works.
Results:
In August 2024, the first phase of the enhanced patient transition process rolled out with streamlined EPIC documentation allowing any staff member to easily locate what stage of the transition process the patient is currently in.
Conclusion:
By the end of 2024, the CBT and core process framework will be finalized. All staff who are part of the transition process will complete the CBT. The pediatric-to-adult transition at Children’s Health will be standardized across ambulatory with documentation being efficiently located.
-

Evaluation of Supplemental Oxygen Use in the Acute Care Cardiology Unit and Opportunities for Standardizing Practice
Melanie Walsh, Alexandra Birely, Sarah Mahmalji, and Sonali S. Patel
RESEARCH
Purpose:
Oxygen delivery via nasal cannula is a standard therapy in hospitalized pediatric patients; however, it can have adverse effects in certain populations, such as infants with cardiac shunting physiology1,2. An oxygen-air blender can be used via standard nasal cannula to provide the lowest amount of fraction of inspired oxygen (FiO2) in order to reduce harm2. A recent Pediatric Acute Care Cardiology Collaborative (PAC3) Hospital Survey indicates that 88% of participating acute care cardiology units (ACCU) provide blended oxygen to patients, however, indications for use are not well-established3,4. A local ACCU nursing staff survey revealed mixed use of blended oxygen and variable understanding of current oxygen weaning orders and protocols. A literature search did not provide sufficient guidance on oxygen use best practices in patients with congenital heart disease. We sought to evaluate the current practice of oxygen administration in our ACCU.Project Design:
Data extraction from PAC3 registry for local ACCU encounters on oxygen use for patient encounters since October 2021. Multidisciplinary group convened to outline patient and data field inclusion criteria. Data evaluated for all ACCU encounters for patients on supplemental oxygen via nasal cannula. A gap analysis and a process map were utilized to better understand the current state.Results::
ACCU patient encounters used supplemental oxygen, of which 14.6% utilized blended oxygen. Analysis revealed confusion of electronic medical record (EMR) oxygen weaning led to varying approaches for choosing amount of flow versus amount of concentrated oxygen (FiO2) as the weaning mechanism. Additional causes included standard use of blenders in the cardiovascular intensive care unit, a knowledge gap of the proper indication for blended oxygen, and lack of guidelines for weaning oxygen.Conclusion:
Best practice guidelines nor standard oxygen weaning protocol exist for blended oxygen use in patients with congenital heart disease. Future steps include analysis of patient-specific factors related to the use of blended oxygen to establish best practice guidelines.References:
1. Dietrich Klauwer, Christoph Neuhaeuser, Josef Thul, & Rainer Zimmermann. (2019). A Practical Handbook on Pediatric Cardiac Intensive Care Therapy. Springer.
2. Walsh, B. K., & Smallwood, C. D. (2017). Pediatric oxygen therapy: a review and update. Respiratory care, 62(6), 645-661.
3. Hoerst, A., Bakar, A., Cassidy, S. C., Clabby, M., Grippo, E. D., Graupe, M., ... & Pediatric Acute Care Cardiology Collaborative (PAC3). (2019). Variation in care practices across pediatric acute care cardiology units: Results of the Pediatric Acute Care Cardiology Collaborative (PAC3) hospital survey. Congenital Heart Disease, 14(3), 419-426.
4. Pediatric Acute Care Cardiology Collaborative (PAC3) hospital survey, Version 3.0. -

Got Questions? Call us: Utilizing Telephone Triage to Help Pediatric Patients After Discharge
Susan Webber and Ann Gosdin
EBP
Background: Discharge follow-up programs help to reduce avoidable readmissions and unnecessary returns to the emergency department. Our organization lacked a clearly defined post-inpatient discharge process for patients on the hospitalist service. Information on the after-visit summary (AVS) includes follow-up appointment instructions and lists the main hospital phone number. Primary care providers often refer patients back to the hospital for questions related to the hospital stay. Post-discharge follow-up phone calls are labor-intensive, hard to sustain, and may not meet the patient’s needs. We sought a technology solution to assist and engage families post-discharge.
Purpose: This project aims to determine if patient-initiated calls to experienced triage nurses in a 24/7 centralized call center can identify barriers and assist with self-management at home.
Implementation: Leveraging technology and a new AVS phone number workflow, we implemented a pilot program to engage patients after discharge in January 2021. Patients discharged from the hospitalist service received a standardized text message script comprising seven discharge-related questions. In the technology solution, responses to the text questions either prompt the user to connect with the Nurse Advice Line (NAL) or move to the next question. The phone system identifies calls originating from either discharge method, and lines are open 24/7. In January 2022, the NAL partnered with Care Coordination. Symptom-based calls route to the NAL for triage 24/7, and all other call types route to the NAL after business hours.
Outcomes: In 2023, the hospitalist service discharged 2,305 patients.
For Quarter 1 of 2023, the NAL managed 95 calls. Of those, 56 had new or worsening symptoms, 24 had a medication issue or questions about their medications, and three had questions about their discharge instructions. The remaining had inquiries about durable medical equipment, general information, work or school notes, and follow-up appointments.
For Quarter 2 of 2023, the NAL managed 220 calls. Of those, 144 had new or worsening symptoms, 51 had a medication issue or questions about their medications, five had questions about their discharge instructions, and the remaining DME, general information, work or school notes, and follow-up appointments.
Of the 315 patient calls for 2023, 39 patients required readmission.
Relevance: This poster will enable the learner to understand why pediatric patients call after hours and meet them at their time of need for prompt answers.
- Binder, Andrew B. and Donald F. Cox. “Changes in Health Care Costs and Mortality Associated with Transitional Care Management Services after a Discharge among Medicare Beneficiaries.” JAMA Internal Medicine 178.9 (2018):1165-1171
- Bressman, Eric, MD, MSHP: Judith A. Long, MD and Katherine Honig, et al. “Evaluation of Automated Text Message-Based Program to Reduce Use of Acute Health Care Resources after Discharge.” doi:10.1001/jamanetworkopen.2022.38293
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.







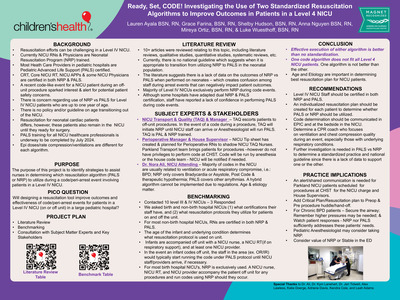{kind=link}
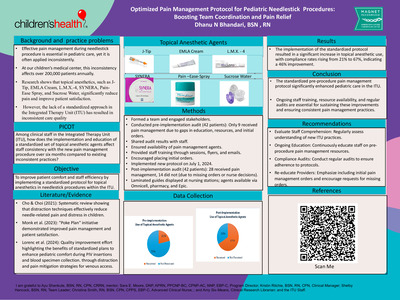{kind=link}
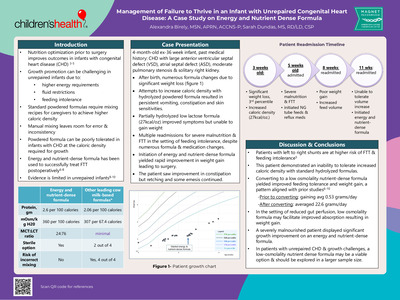{kind=link}
{kind=link}
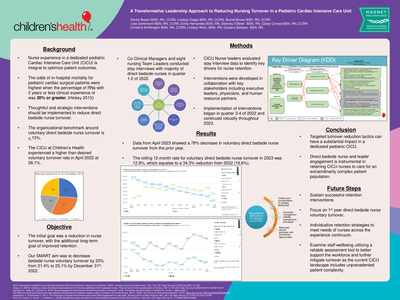{kind=link}
{kind=link}
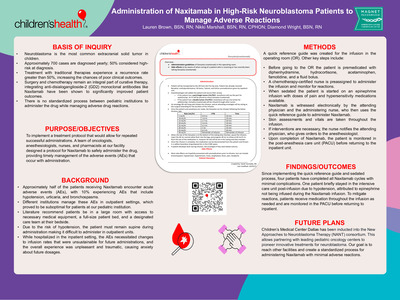{kind=link}
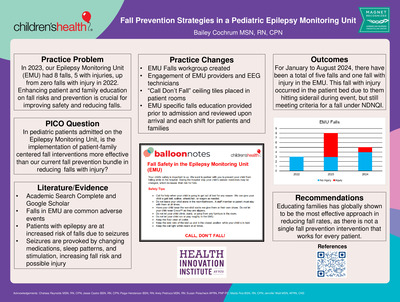{kind=link}
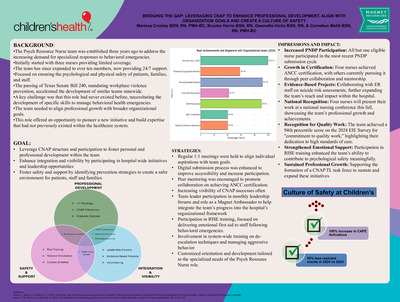{kind=link}
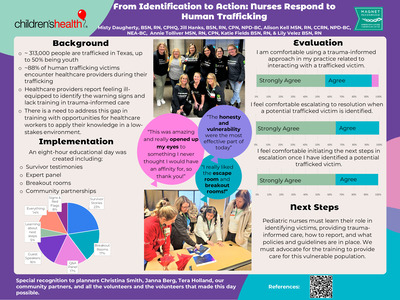{kind=link}
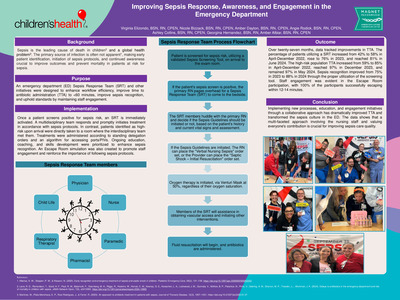{kind=link}
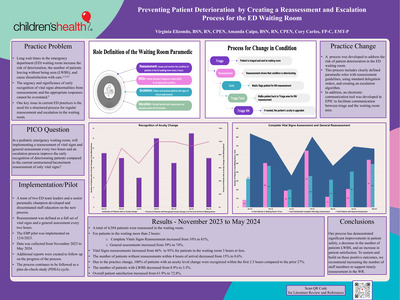{kind=link}
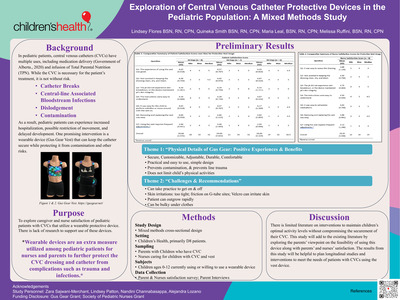{kind=link}
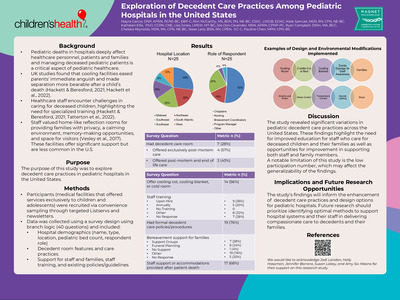{kind=link}
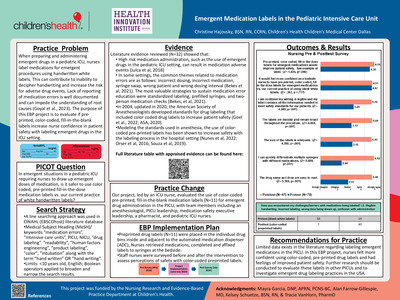{kind=link}
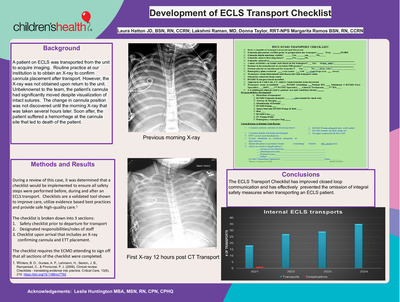{kind=link}
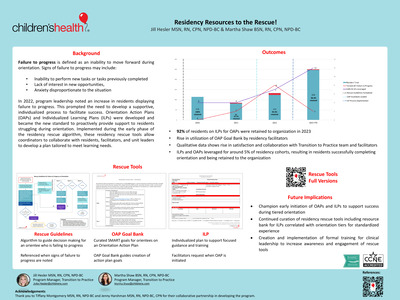{kind=link}
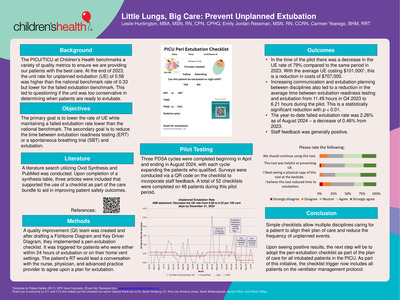{kind=link}
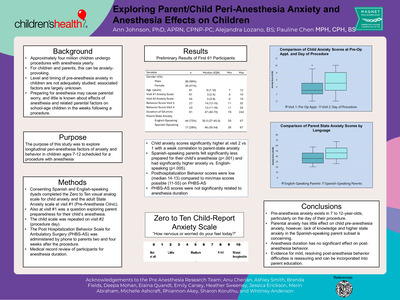{kind=link}
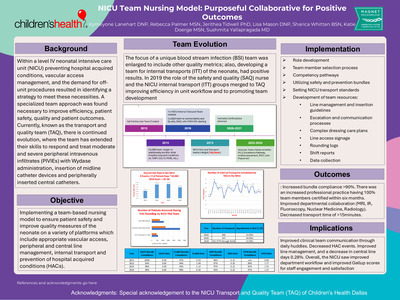{kind=link}
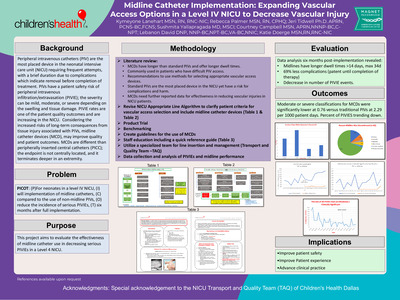{kind=link}
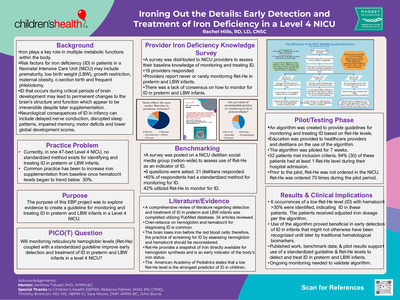{kind=link}
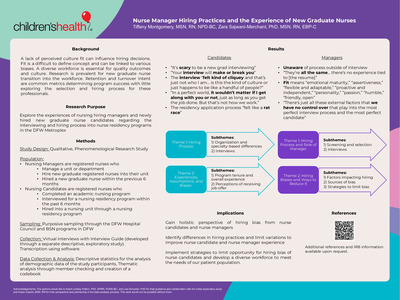{kind=link}
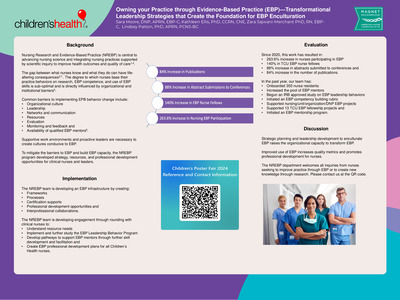{kind=link}
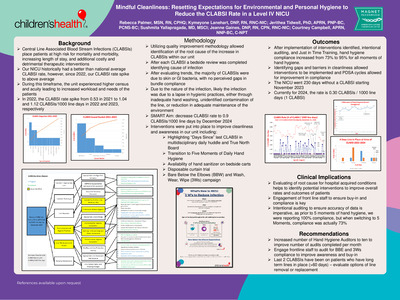{kind=link}
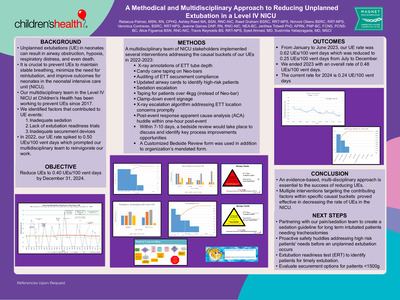{kind=link}
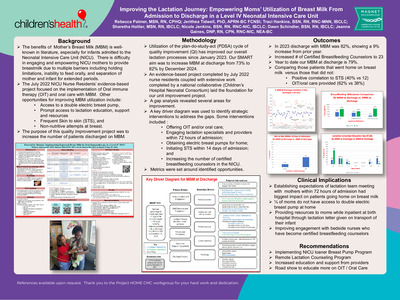{kind=link}
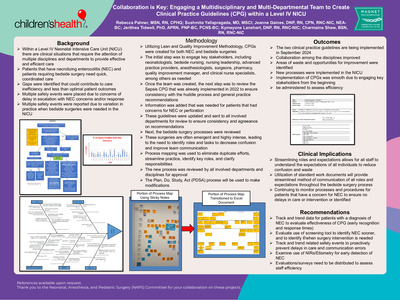{kind=link}
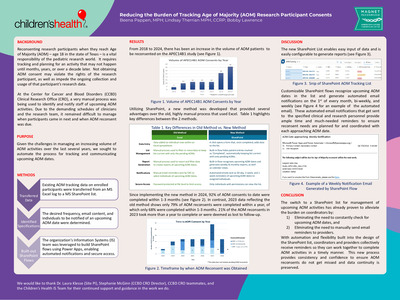{kind=link}
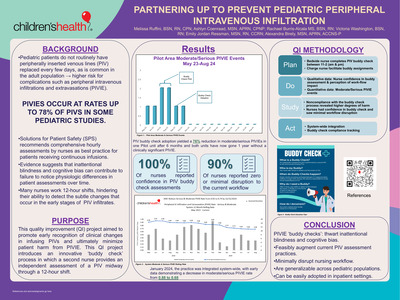{kind=link}
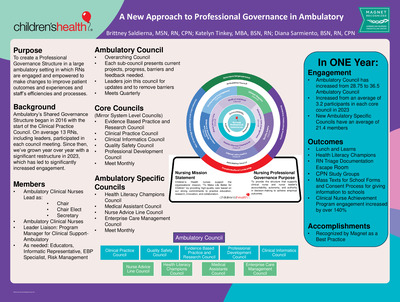{kind=link}
{kind=link}
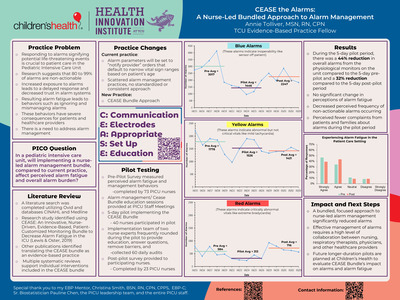{kind=link}
{kind=link}
{kind=link}
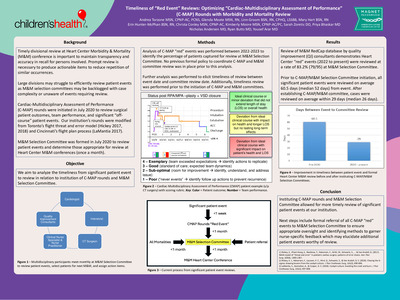{kind=link}
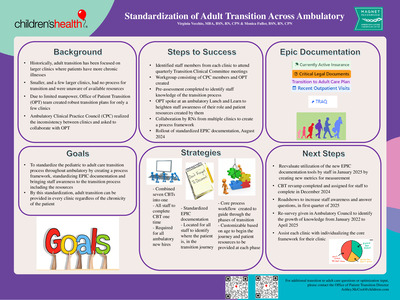{kind=link}
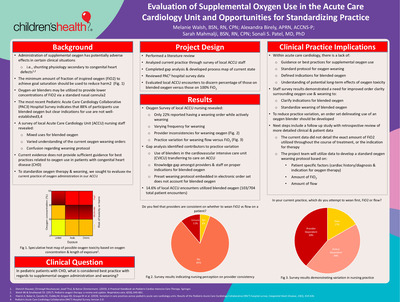{kind=link}
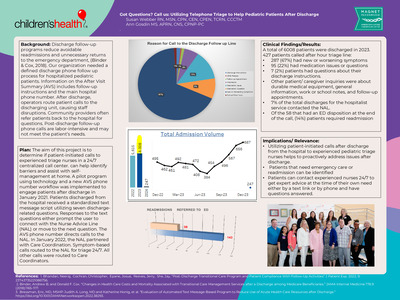{kind=link}