

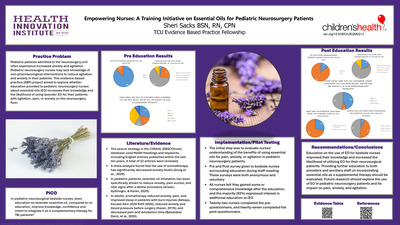
-

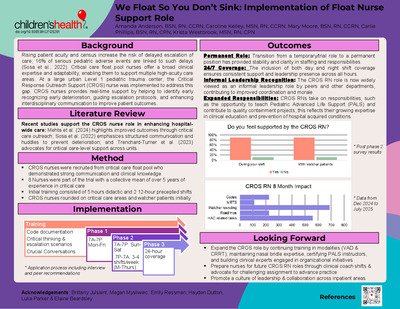
We Float So You Don’t Sink: Implementation of Float Nurse Support Role
Amanda Anderson, Caroline Kelley, Mary Moore, Carlie Phillips, and Krista Westbrook
INNOVATION & LEADERSHIP
Background: Critical care float pool nurses possess broad clinical expertise and flexibility to support a wide range of patient care areas across the organization. Their familiarity with multiple units, patient populations, and
established relationships with provider teams helps them to facilitate timely and effective clinical support. Acute care staff regard critical care nurses’ judgment with high respect, enhancing interdisciplinary collaboration and trust. Because of a rising patient acuity and census, there is risk for failures in escalation of care, with 16% of serious pediatric adverse events linked to delays is escalation (Sosa et al., 2022). Critical care nurses can play a pivotal role in supporting bedside teams and reinforcing escalation protocols, as evidenced by proactive rounding on “watchers,” high risk patients. This positions these nurses to uniquely enhance escalation pathways and contribute to improved patient outcomes.Implementation: In a large urban free-standing Level 1 pediatric trauma center, the Critical Response Outreach Support (CROS) nurse was developed to support nurses in early recognition and intervention, escalation processes, and team communication. This role was piloted over six months using experienced critical care float pool nurses in a phased approach. Prior to go-live, these nurses attend a comprehensive training program that consists of didactic lectures, simulated code documentation, and a hospital-wide scavenger hunt designed to enhance familiarity with the institution and the placement of critical resources such as crash carts and automated external defibrillators. CROS nurses served as clinical mentors, assisted with escalation events, and contributed to hospital-acquired condition prevention.
Evaluation: Preliminary outcomes for this role are very positive with nurses reporting a high level of real-time support and education, with 89% stating there is value in this role. This role also supported early controlled transfer of patients, so interventions could be started proactively, with only 3 of 67 controlled transfers needing a further level of escalation of care upon arrival to the intensive care unit. Given the success of the CROS role, it is being fully implemented to support nurses and patient safety. The CROS nurse represents a scalable, evidence-informed strategy to improve pediatric patient outcomes while fostering a culture of continuous learning and interdisciplinary collaboration.
-

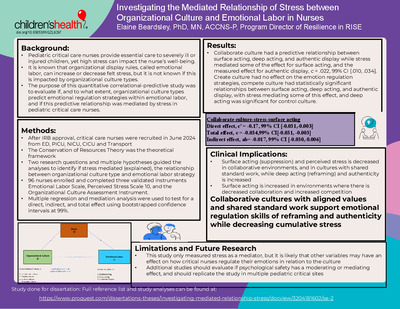
Investigating the Mediated Relationship of Stress between Organizational Culture and Emotional Labor in Nurses
Elaine Beardsley
RESEARCH
Purpose: Pediatric critical care nurses provide essential care to severely ill or injured children, yet high stress can impact the nurse’s well-being. Although it is known that exposure to traumatic events can contribute to secondary trauma for the nurse, it is becoming more widely understood how the work environment is a contributing factor on how stress is experienced by the nurse. It is also known that emotion regulation strategies to meet organizational display rules, called emotional labor, can increase or decrease felt stress, but it is not known if this is impacted by organizational culture types. The purpose of this quantitative correlational-predictive study was to evaluate if, and to what extent, organizational culture types predict emotional regulation strategies within emotional labor, and if this predictive relationship was mediated by stress in pediatric critical care nurses. The Conservation of Resource Theory was used to guide the research questions and related hypotheses.Methods: After IRB approval was received, recruitment began in June 2024 with the registered nurses from Transport, and the Critical Care Units and Emergency Departments in Dallas and Plano. Three validated instruments were used to collect data from 96 pediatric critical nurses, which included the Emotional Labor Scale, Perceived Stress Scale 10, and the Organizational Culture Assessment Instrument. RQ1 investigated if there was a predictive total effect between the organizational culture type (collaborate, create, compete, control) and the emotional regulation strategy used in emotional labor (surface acting, deep acting, authentic display). RQ2 investigated whether the indirect effect between organizational culture type and emotional regulation strategy in emotional labor was mediated by cumulative stress. Multiple regression and mediation analysis were used to test for a direct, indirect, and total effect using bootstrapped confidence intervals at 99%.
Results: There were statistically significant relationships between organizational culture types and the emotion regulation strategy within emotional labor, but it depended on the variable. The results showed that depending on the culture type, surface acting (suppression) decreased while deep acting (reframing) increased, some of which were mediated by stress levels. Collaborate culture had a predictive relationship between surface acting, deep acting, and authentic display while stress mediated some of the effect for surface acting, and all the measured effect for authentic display. Create culture had no effect on the emotion regulation strategies in emotional labor. Compete culture had statistically significant relationships between surface acting, statistically significant relationships between surface acting, deep acting, and authentic display, with stress mediating some of this effect. These results confirm the importance of healthy work environments, and give suggestions for improvement
-

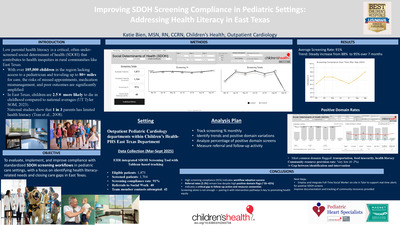
Improving SDOH Screening Compliance in Pediatric Settings: Addressing Health Literacy in East Texas
Katie Bien
QUALITY IMPROVEMENT
Background: Low parental health literacy is an under-screened social determinant of health (SDOH) that drives inequities in rural communities such as East Texas, where over 105,000 children lack access to a pediatrician, and families travel 80+ miles for care. Pediatric mortality in this region is 2.5 times the national average (UT Tyler SOM, 2023). National data indicate that one in three parents has limited health literacy (Tran et al., 2008), further exacerbating risks of missed appointments, medication errors, and poor outcomes.Methodology: The initiative was conducted in a rural outpatient pediatric cardiology clinic within Children’s Health located in Tyler, Texas (PHS Tyler). Tyler is a small town with a population of approximately 108,000, 95 miles southeast of Dallas, Texas- the main hospital campus. After Children’s inpatient areas implemented SDOH screening in 2021, the project was expanded to the Outpatient areas. PHS Tyler was an early outpatient adopter motivated to deploy resources to patients and families. Strategies implemented included monthly compliance monitoring, staff training, and workflow reinforcement. With the deployment of an EHR-integrated SDOH screening tool, a resource page was developed with a list of local community resources like the food bank, housing resources, and WIC enrollment information. PHS Tyler utilized Tableau dashboards and tracked compliance from March-September 2025. Eligible patients (n=1,873) were included.
Outcomes: SDOH workflow integration consisted of the use of an iPad in the clinic and MyChart questionnaires prior to their appointment resulting in staff reported satisfaction, engagement, and ease. Consistent leadership follow-up with staff and social work involvement also contributed to improved engagement with the screening process. Screening compliance increased steadily, rising from 88% in March to 91% in September. Across the seven-month period, compliance averaged 91% (range 88–95%). Positive screens were identified in 35–42% of encounters, with the most common domains being transportation, food insecurity, and health literacy.
-

Advancing Cardiorespiratory Care in the Heart Center: Development of a Specialized Cardiac Curriculum for Respiratory Therapists
Alexandra Birely, Andrea Torzone, Jill Kleiber, Elysia Harshman, and Melinda Cory
INNOVATION & LEADERSHIP
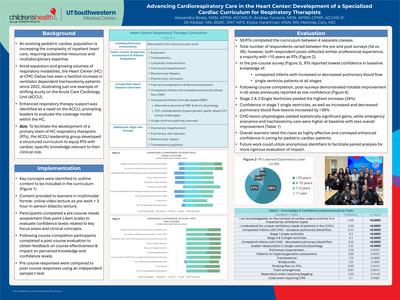
Background: As innovations advance the outcomes and survival of pediatric patients with heart disease, an evolving patient population is increasing the complexity of inpatient heart care. The Heart Center at Children’s Health Dallas has seen a twofold increase in ventilator dependent tracheostomy patients since 2022, illustrating just one example of the shifting acuity profile of patients being cared for on the Acute Care Cardiology Unit (ACCU). Providing safe and high-quality care within a pediatric Heart Center requires enhanced resources and expertise across the entire multidisciplinary team. The need for increased respiratory therapy support was identified on the ACCU amid unit expansion and growing volumes of respiratory modalities. To facilitate the development of a primary team of Heart Center respiratory therapists (RTs), the leadership group aimed to develop a curriculum of cardiac content pertinent to respiratory care provision.Implementation: Key concepts were identified to outline the structure for content to be included in the curriculum. Content was compiled and provided to learners in multimodal format consisting of an online video lecture to be completed as pre-work and a 3 hour in-person didactic lecture. Participants completed a pre- and post- course survey to evaluate self-reported confidence levels related to key focus areas and clinical concepts.
Evaluation: In the baseline pre-course survey, respiratory therapists reported lowest confidence in baseline knowledge of unrepaired infants with increased or decreased pulmonary blood flow and managing sudden desaturation in single ventricle patients. Following course completion, post-surveys demonstrated notable improvement in the areas previously reported as low confidence. Stage 2 & 3 Single Ventricles yielded the highest increase (37%) along with increased and decreased pulmonary blood flow lesions. Confidence in caring for stage 1 single ventricles increased by 33%. Overall learners rated the class as highly effective and conveyed enhanced confidence in caring for pediatric cardiac patients. To date, the first of 4 scheduled classes have been conducted with additional results to be analyzed upon completion of all classes.
-

Comparing In-Person Discussions Versus Online Learning Modules on Post-PDA Ligation Care Knowledge Retention Among Night Shift Nurses in a Level 4 NICU
Jeffrey Canlas, Olga DeLeon, Sharon Summers, Jerithea Tidwell, and Noorjahan Ali
QUALITY IMPROVEMENT
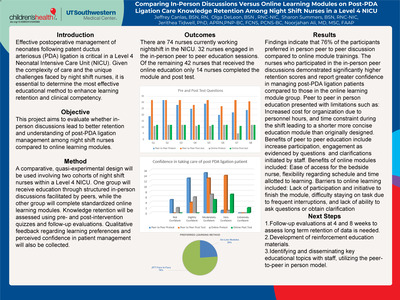
Background: Postoperative management of neonates following patent ductus arteriosus (PDA) ligation is critical in a Level 4 Neonatal Intensive Care Unit (NICU). Night shift nurses are faced with unique challenges when caring for these patients. The night shift NICU leaders wanted to determine the most effective educational method to enhance learning retention and clinical competency. The purpose of this quality improvement project was to evaluate whether in-person discussions lead to better retention and understanding of post-PDA ligation management among night shift NICU nurses compared to online learning modules.Methodology: A comparative, quasi-experimental design was used to compare knowledge retention and clinical competency between two cohorts of night shift nurses. One group received education through structured in-person discussions facilitated by peers, while the other group completed a standardized online learning modules. Pre- and post-intervention quizzes and follow-up evaluations were administered to both groups.
Outcomes: 74 nurses participated in the project. Results revealed limitations and benefits for both methods. A significant difference in clinical competency was found. 76% of the participants preferred in person peer to peer discussion compared to online module trainings.
-

Epilogue: Postoperative 30-Day Follow-Up
Tess Davis, Karisa Price, and Courtney Russ
INNOVATION & LEADERSHIP
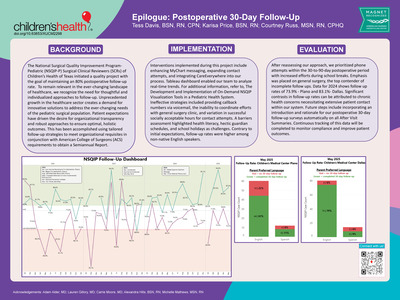
Background: The NSQIP-P Surgical Clinical Reviewers (SCR) of Children’s Health of Texas initiated a quality project with the goal of maintaining an 80% postoperative follow-up rate. To remain relevant in the ever-changing landscape of healthcare, we recognize the need for thoughtful and individualized approaches to follow-up. Unprecedented growth in the healthcare sector creates a demand for innovative solutions to address the ever-changing needs of the pediatric surgical population. Patient expectations have driven the desire for organizational transparency and robust approaches to ensure optimal, holistic outcomes. This has been accomplished using tailored follow-up strategies to meet organizational requisites in conjunction with American College of Surgeons requirements to obtain a Semiannual Report.Implementation: Interventions implemented during this project include enhancing MyChart messaging, expanding contact attempts, and integrating CareEverywhere into our process. Tableau dashboard enabled us to analyze real-time trends. For additional information, refer to, The Development and Implementation of On-Demand NSQIP Visualization Tools in a Pediatric Health System. Ineffective strategies included providing callback numbers via voicemail, the inability to coordinate efforts with general surgery clinic, and variation in successful socially acceptable hours for contact attempts. A barriers assessment highlighted health literacy, hectic guardian schedules, and school holidays as challenges. Contrary to initial expectations, follow-up rates were higher among non-native English speakers.
Evaluation: After reassessing our approach, we prioritized phone attempts within the 30-to-90-day postoperative period with increased efforts during school breaks. Emphasis was placed on general surgery, the top contender of incomplete follow ups. Data for 2024 shows follow up rates of 73.9% - Plano and 83.1%- Dallas. Significant contrasts in follow-up rates can be attributed to chronic health concerns necessitating extensive patient contact within our system. Future steps include incorporating an introduction and rationale for our postoperative 30-day follow-up surveys automatically on all After Visit Summaries. Continuous tracking of this data will be completed to monitor compliance and improve patient outcomes. -

The Development and Implementation of On-Demand NSQIP Visualization Tools in a Pediatric Health System
Tess Davis, Karisa Price, and Courtney Russ
INNOVATION & LEADERSHIP
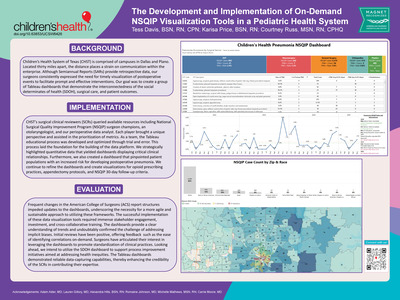
Background: Children’s Health System of Texas (CHST) is comprised of campuses in Dallas and Plano. Located thirty miles apart, the distance places a strain on communication within the enterprise. While Semiannual Reports (SARs) provide retrospective data, our surgeons frequently voiced a desire to visualize timely postoperative occurrences in an attempt to provide on-time interventions.Implementation: Surgical Clinical Reviewers (SCRs) queried available resources including National Surgical Quality Improvement Program (NSQIP) surgeon champions, an otolaryngologist, and our perioperative data analyst. Each player brought a unique perspective and assisted in prioritizing metrics. As a team, the Tableau educational process was developed and optimized. This process laid the foundation for the building of the data platform. We highlighted quantitative data in an advantageous manner that yielded dashboards displaying clinical relationships. Furthermore, we were also able to create a dashboard that pinpointed patient populations with an increased risk for developing postoperative pneumonia. We continue to refine dashboards and create visualizations for opioid prescribing practices, appendectomy protocols, and NSQIP 30-day follow-up criteria.
Evaluation: Timely updates to dashboards were hindered by frequent changes in ACS report structures, emphasizing the need for agile and sustainable reporting frameworks Successful implementation of data visualization tools required immense stakeholder engagement, investment, and cross-collaborative training Dashboards provide a clear understanding of trends and confirmed the challenge of addressing implicit biases
-

Advocating for Health Equity: A quality Improvement Project Surrounding Social Determinants of Health Screening
Rose Anne Dela Cruz, Amanda Marquez, and Madison Lemmons
INNOVATION & LEADERSHIP
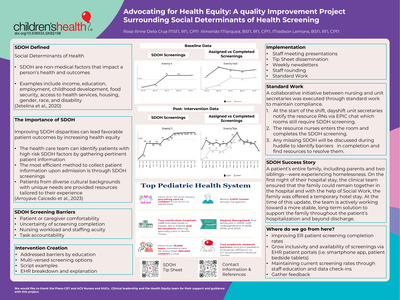
Background: Social Determinants of Health (SDOH) can gravely impact patient recovery. Health organizations should prioritize identifying high-risk SDOH patients to improve patient outcomes. Current research suggests SDOH screening should be standard practice in preventative care. With this awareness, healthcare team members must identify patients with complex social determinants of health needs to ensure essential resources are offered to enhance their healing process during hospitalization and sustain it post-discharge. The most straightforward approach to identifying patients from diverse backgrounds with SDOH requirements is via SDOH screening. The collaborating health system, serving a diverse pediatric population in the northern Texas region, reported a low screening compliance rate of 54% during the initial implementation in February 2024. The Acute Care Department's objective was to improve the screening rate to 85% within a six-month timeframe.Implementation: In July 2025, crowd-sourced feedback identified barriers such as staff comprehension and familiarity with the screening process, navigation of electronic health records, and a family's openness to transparency. To enhance screening compliance from the baseline of 59% to the target of 85%, bedside staff and leadership educational workgroup created and deployed a screening barrier tip sheet. In August 2024, the "tip sheet" was disseminated during staff meetings, leader-staff rounding, and weekly newsletter. It had descriptive verbiage for bedside staff to use when describing the screening to families, along with different ways to complete it, such as conversing, using a tablet, or using MyChart, to name a few. Following the implementation of the tip sheet, screening percentages increased to >90% in December 2024. A collaboration between nursing staff and health unit coordinators was implemented to maintain compliance percentages, resulting in a 96% compliance rate as of May 2025.
Evaluation: Patients who previously had unmet needs now have access to services like stable housing as screening percentages rise. Moreover, patients from diverse backgrounds with unique needs receive resources tailored to their experiences. To further the development of the SDOH screening tool, it is essential to implement screenings in more patient care settings, such as the emergency department, and to establish a notification system for patients and caregivers to complete the screening. Utilizing an SDOH screening tool enables nurses to enhance health equality, thus creating a foundation for access to high-quality care.
-

Reducing Unexpected Nasogastric Tube Reinsertions Through Interdisciplinary Education: A Pediatric Ambulatory Initiative
Jordon Delatorre, Nadia Gose, Leslie Moore, Aren Parker, Shivani Patel, and Iman Rahim-Tejani
INNOVATION & LEADERSHIP
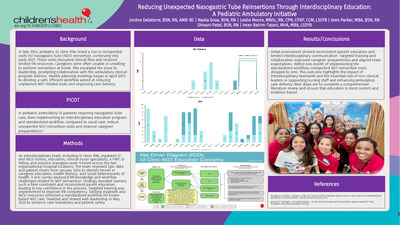
Background: In late 2024, pediatric GI clinic RNs noted a rise in unexpected visits for nasogastric tube (NGT) reinsertion, continuing into early 2025. These visits disrupted clinical flow and strained limited RN resources. Caregivers were often unable or unwilling to perform reinsertion at home. RNs escalated the issue to leadership, prompting collaboration with the ambulatory clinical program director. Weekly planning meetings began in April 2025 to develop a safe, efficient workflow aimed at reducing unplanned NGT-related visits and improving care delivery.Implementation: An interdisciplinary team, including GI clinic RNs, inpatient GI and NICU nurses, educators, clinical nurse specialists, A PNP, GI fellow, and practice managers were formed across the two organizational hospital locations. The team reviewed Epic data and patient charts from January 2024 to identify trends in caregiver education, health literacy, and social determinants of health. A pre-survey assessed RN knowledge and workflow challenges related to NGT reinsertion. Findings revealed barriers such a time constraint and inconsistent parent education, leading to low confidence in the process. Targeted training was implemented to improve RN competency. Existing inpatient and NICU resources informed a standardized workflow for home-based NGT care, finalized and shared with leadership in May 2025 to enhance care transitions and patient safety.
Evaluation: Initial assessment showed inconsistent patient education and limited interdisciplinary communication. Targeted training and collaboration improved caregiver preparedness and aligned team expectations. Within one month of implementing the standardized workflow, unexpected NGT reinsertion visits dropped to zero. This outcome highlights the impact of interdisciplinary teamwork and the essential role of non-clinical leaders in supporting nursing staff and enhancing ambulatory care delivery. Next steps are to complete a comprehensive literature review and ensure that education is more current and evidence based.
-

Bibbidi-Bobbidi No Boo-boo Pulse-Oximeter: A Child-Friendly Prototype to Improve the Pediatric Experience
Holly Dickens
INNOVATION & LEADERSHIP
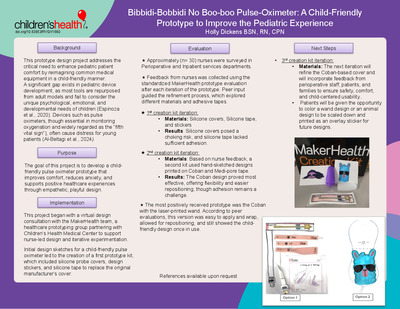
Background: This prototype design project addresses the critical need to enhance pediatric patient comfort by reimagining common medical equipment to be child-friendly. A significant gap exists in pediatric device development, as most tools are repurposed from adult models and fail to consider the unique psychological, emotional, and developmental needs of children (Espinoza et al., 2020). Devices such as pulse oximeters, though essential in monitoring oxygenation and widely regarded as the “fifth vital sign” (Al-Beltagi et al., 2024), often cause distress for young patients. Traditional models feature intimidating adult-centric aesthetics, bright red sensor lights, and sticky wraps that are uncomfortable and easily removed, creating frustration for both children and caregivers (Williams, 2009). The goal of this project is to develop a child-friendly pulse oximeter prototype that improves comfort, reduces anxiety, and supports positive healthcare experiences through empathetic, playful design.Implementation: This project began with a virtual design consultation with the MakerHealth team, a healthcare prototyping group partnering with Children’s Health Medical Center to support nurse-led design and iterative experimentation. Initial sketches for a child-friendly pulse oximeter led to a first prototype kit including silicone probe covers, design stickers, and silicone tape to replace the original manufacturer cover. Testing showed a need for iteration: silicone covers posed choking risks, and silicone tape lacked adhesion. Based on nurse feedback, a second kit used hand-sketched designs printed on Coban and Medi-pore tape. The Coban design proved most effective, offering flexibility and easier repositioning, though adhesion remains a challenge. The next iteration will refine the Coban-based cover by adding glue dots for stability and will incorporate feedback from perioperative staff, patients, and families to ensure safety, comfort, and child-centered usability.
Evaluation: Feedback from nurses in the peri-operative department was collected using the standardized MakerHealth prototype evaluation after each prototype iteration. Peer input guided the refinement process to explore different materials and adhesive tapes. The most positively received prototype was the Coban with the laser-printed wand. According to peer evaluations, this version was easy to apply and wrap, allowed for repositioning, and still showed the child-friendly design once in use. The next prototype iteration will include wand designs that developed by patients to increase their pediatric appeal and will continue to seek evaluation feedback from staff and families. References available upon request.
-

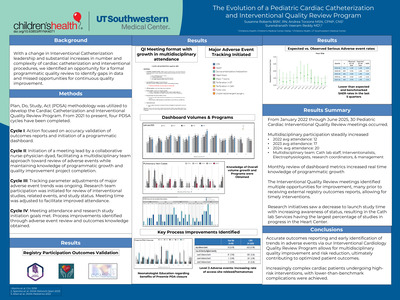
A Nurse-Led Investigation into Rising Cardiology Clinic Admission Holds and a Multidisciplinary Strategy to Reduce Them
Jennifer Dickson, Haley Byrne, Katherine Harris, and Leah K. Toombs
INNOVATION & LEADERSHIP
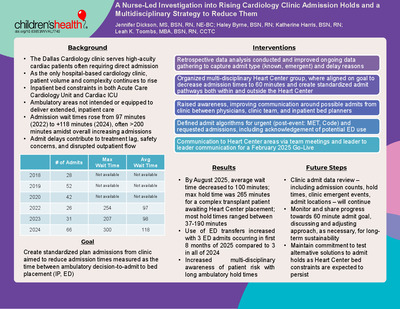
Background: The Dallas Cardiology Clinic, the only hospital-based clinic within the Heart Center’s outpatient network, serves specialized, high-acuity cardiac patients who often require direct admission. Due to inpatient bed constraints in the Acute Care Cardiology Unit and Cardiac ICU, rising patient complexity, patients are increasingly held in the ambulatory space, not intended for, or equipped for prolonged care. In 2024, average admission wait times rose to 118 minutes (often taking 200+ minutes) up from 97 minutes in 2022. Long admit wait times can lead to treatment delays, raise nursing concerns about safety, and disrupt outpatient flow. A gap in standardized admission approaches for both anticipated clinic admits and urgent patient event admissions. In response, a nurse-led initiative analyzed retrospective data to build consensus on the problem and organize a Heart Center -wide approach to improve timely, patient-centered transfers.Implementation: A multidisciplinary Heart Center group aligned around gaps in the clinic admission process and the shared aim to reduce admission times (decision-to-admit to inpatient bed placement). Clinic admit data from 2018 was assessed with initial intervention to solidify data gathering in 2024 ensuring all admit type (known and emergent) and delay reasons were captured. As inpatient ADC continues to increase, the team recognized the need to develop standardized, scalable pathways utilizing bed locations both within the Heart Center and utilization of ED when beds are not readily available. Key improvements included enhanced communication around clinic admit potential to both the clinic team and inpatient bed planners; agreement in 60 minutes as a safe wait time for bed placement; and defined admit algorithms for urgent (post-event) and requested admissions. Go-live was Feb 2025; communication to Heart Center areas was initiated via team meetings and leader to leader communication.
Evaluation: Cardiology clinic admission data from 2018–2024 showed rising demand and wait times due to limited inpatient bed availability. In 2024, 66 admissions occurred with an average wait of 118 minutes. Maximum waits of 300 minutes happened multiple times, with only three patients transferred to the ED. By August 2025, average wait time decreased to 100 minutes. A transplant admission experienced a 265-minute wait, though most holds ranged from 37–190 minutes. ED transfers increased, with three occurring in the first eight months of 2025. These shifts reflect growing awareness of risks tied to prolonged ambulatory holds and a commitment to testing alternative solutions, as Heart Center bed constraints are expected to persist. Ongoing data review—including admission counts, hold times, and clinic emergent events—continues. Early findings suggest reduced delays and improved team coordination. Monitoring will assess progress toward the 60-minute transfer target and long-term sustainability.
-

From Competence to Confidence: Fostering a Culture of Certification in Nursing
DeRhonda Dossett, Sunni Fleming, Amanda Grantham, and Johanna Muller
INNOVATION & LEADERSHIP
Background: Nursing certifications help promote excellence in nursing and support the professional identity of nurses. In an urban academic pediatric hospital system, nursing leaders were tasked with increasing professional nursing certification rates within their departments. One team has excelled in increasing their professional certification rate. The team went from 8 to 35 certified nurses which was a 33.75% increase from July 2022 to July 2025. This has elevated the confidence and knowledge base of the nurses and leaders in the Variable Staffing department. Objectives included increasing knowledge and awareness of professional certification, providing resources available to assist with obtaining a certification, and increasing the number of certified nurses within the Variable Staffing department.Implementation: Leading by example, five team leaders obtained their first certification and the director attained a second certification during this time frame. This encouraged staff to also obtain their certifications. Department leadership worked with the Unit Practice Council to create a goal of increasing the department’s certification rate. The Unit Practice Council created a virtual page with certification resources. A presentation was also made to the new graduate nursing group that would reach certification eligibility within the next few months. Variable staffing leaders assisted with creating and presenting content for system-wide certification study circles. They also saw a need for increased flexibility with review courses, so a virtual Certified Pediatric Nurse review course was created and is ongoing. Once Variable Staffing nurses obtained their certifications, leaders provided special recognition in multiple avenues.
Evaluation: The department started with 8 nurses with professional certifications in 2022. As of July 2025, the department has a total of 35 nurses with professional certifications. Certifications range from pediatric, pediatric emergency, pediatric critical care, neonatal, and executive leadership. The department experienced a 33.75% increase in certified nurses. The Variable Staffing department was able to significantly increase the percentage of certified nurses by providing information and resources for certification as well as recognition after they pass the certification exam. This helped advance the professional identity of nurses within the department as well as the leaders.
-

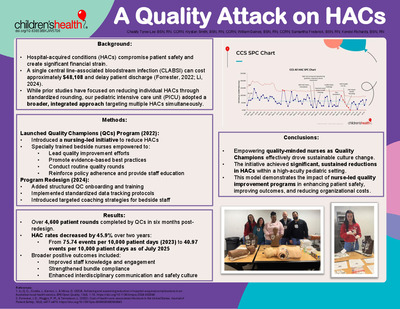
Walk the Talk: Elevating Quality One Step at a Time
Hayden Dutton, Jesse Castro, Maria Leal, and Megan Mysliwiec
QUALITY IMPROVEMENT
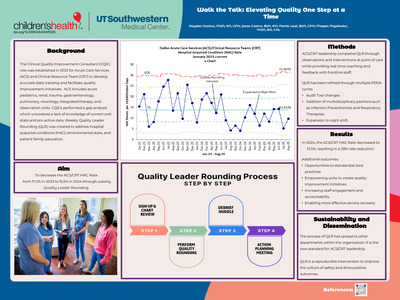
Background: The Clinical Quality Improvement Consultant (CQIC) role was established in 2023 for Acute Care Services (ACS) and Clinical Resource Teams (CRT). This role was developed to accurately track data and facilitate quality improvement initiatives. ACS includes acute pediatrics, renal, trauma, gastroenterology, pulmonary, neurology, integrated therapy, and observation units. CQICs performed a gap analysis which uncovered a lack of knowledge of current unit state and pro-active hospital acquired condition (HAC) data. In partnership with clinical leaders, a weekly Quality Leader Rounding (QLR) was created to address this, environmental state, and patient family education. The goal of QLR was to decrease the HAC Rate for the included units from 17.2% in 2023 to 15.5% in 2024.Methodology: The leadership team completes QLR through observations and interventions at point of care while providing real time coaching and feedback with frontline staff. QLR has been refined through multiple PDSA cycles, including changes to the audit tool, lessons learned to add multidisciplinary partners such as Infection Preventionists and Respiratory Therapists and expansion to night shift. After QLR, debrief huddles are held to share immediate findings. In addition, CQIC’s collect and share weekly updates and track monthly progress for ACS/CRT leadership. Action planning meetings are held bi-monthly to address sustained trends and standardize processes.
Outcomes: In 2024, the HAC Rate decreased to 12.5%, exceeding the initial goal and resulting in a 28% rate reduction. This reduction also impacted the system HAC rate which saw a 24% reduction. Additional outcomes included: opportunities to standardize widely valued best practices while also empowering individual units to initiate quality improvement projects; an increase in staff engagement and accountability, fostering an enhanced culture of safety; and an avenue to address patient concerns in real time enabling more effective service recovery. The process of QLR has produced positive outcomes and has spread to other departments within the organization. It is now engrained as standard practice for ACS/CRT leadership. QLR is well supported by the literature as a reproducible intervention that improves the culture of safety and drives positive outcomes.
-

Oh, my Baby! A QI Initiative to Improve Neonatal Thermoregulation Compliance via Nurse-Led Training and Development of a Resource Binder
Gene Mae Estoya, Rose Dela Cruz, and Deb Lathrop
QUALITY IMPROVEMENT
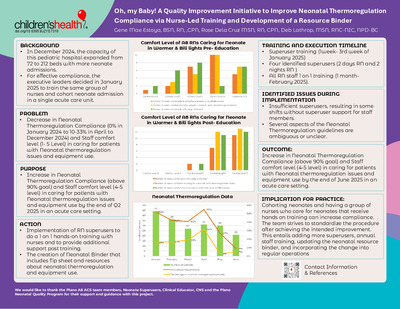
Background: Plan- Problem: Decrease in Neonatal Thermoregulation Compliance (0% in January 2024 to 10-33% in April to December 2024) and Staff comfort level (1- 5 Level) in caring for patients with Neonatal thermoregulation issues and equipment use. Background: In December 2024, the capacity of this pediatric hospital expanded from 72 to 212 beds with more neonate admissions. For effective compliance, the executive leaders decided in January 2025 to train the same group of nurses and cohort neonate admission in a single acute care unit. Goal: Increase in Neonatal Thermoregulation Compliance (above 90% goal) and Staff comfort level (4-5 level) in caring for patients with Neonatal thermoregulation issues and equipment use by the end of Q2 2025 in an acute care setting.Methodology: Do – Implementation of RN superusers to do a 1 on 1 hands-on training with nurses and to provide additional support post training. The creation of Neonatal Binder that includes Tip sheet and resources about neonatal thermoregulation and equipment use. Training Plan and Execution – Superuser training (1week- 3rd week of January 2025) with 4 identified superusers (2 days and 2 nights) then all staff 1 on 1 training (1 month-February 2025). Study / Measure the result- Neonatal compliance data: May 2025 – 97%, June – 95% Pre and post survey – Staff Comfort level in caring for Neonates - Comfort levels improved from a 1- to 5-point range prior to training to a 4- to 5-point range post-training. Identified issues during implementation: Insufficient superusers, resulting in some shifts without superuser support for staff members. Several aspects of the guidelines are ambiguous or unclear.
Outcomes: Act- Cohorting neonates and having a group of nurses who care for neonates that receive hands on training can increase compliance. The team strives to standardize the procedure after achieving the intended improvement. This entails adding more super-users, annual staff training, updating the neonatal resource binder, and incorporating the change into regular operations. Outcome- Increase in Neonatal Thermoregulation Compliance (above 90% goal) and Staff comfort level (4-5 level) in caring for patients with Neonatal thermoregulation issues and equipment use by the end of June 2025 in an acute care setting.
-

Advancing Health Equity Through Comprehensive Haircare Training to Reduce Pediatric Hospital-Acquired Pressure Injuries
Afra Evans, Adrienne Johnson, and Adrienne Davis
QUALITY IMPROVEMENT
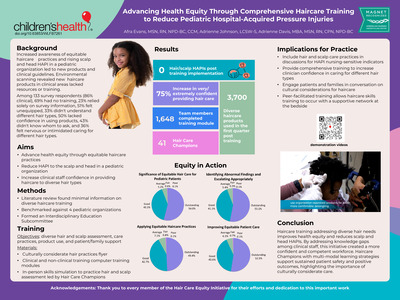
Background: Increased awareness of health equity and a rise in hospital-acquired pressure injuries (HAPIs) to the scalp and head—particularly among pediatric patients with textured hair—prompted a comprehensive initiative at a pediatric healthcare organization. Environmental scanning revealed that while new haircare products had been introduced into clinical areas, staff lacked the training and resources to use them effectively. A current-state analysis survey of 133 staff members (86% clinical) revealed significant gaps: 69% had never received training in diverse haircare, 51% did not feel equipped to provide appropriate care, and 36% felt nervous or intimidated when caring for hair types different from their own. Additionally, 50% lacked confidence in using products, and 43% didn’t know whom to ask for guidance. These findings highlighted the need for a structured, inclusive educational response to improve staff competence and patient outcomes.Methodology: A transdisciplinary education subcommittee was formed, including NPDs, nurses, allied health professionals, instructional designers, and leaders in community relations and patient experience. The education lead, a member of the Haircare Equity Advisory Committee and coauthor of the clinical guidelines, helped guide the initiative. A literature review revealed minimal published training resources on diverse haircare, and benchmarking with four pediatric organizations provided context. The team developed a multi-modal learning strategy aligned with the organization’s mission. This included a culturally considerate flyer, tailored online courses for clinical and non-clinical staff, and 41 Haircare Champions across seven roles and 20+ practice areas. In-person “roadshows” offered low-fidelity simulations to reinforce learning and practice scalp assessments. Testimonial and demonstration videos supported just-in-time learning and sustained improvements in equitable haircare practices.
Outcomes: The initiative led to measurable improvements in staff confidence and patient safety. Post-training evaluations showed increased learner confidence and achievement of learning objectives. Predictive outcomes for trained clinicians rose from 31% to over 90%, reflecting a significant increase in preparedness. Most notably, the organization achieved a 0% rate of scalp and head HAPIs following implementation. The engagement of Haircare Champions and use of multi-modal strategies supported sustained practice improvements. Discussions around nursing-sensitive indicators, such as scalp hygiene and assessment, have increased, contributing to a more culturally competent workforce. In the first quarter post-training, over 3,700 diverse haircare products were used, and 75% of staff reported feeling very or extremely confident in caring for patients with diverse hair types. These results highlight the impact of inclusive education in advancing health equity and improving outcomes.
-

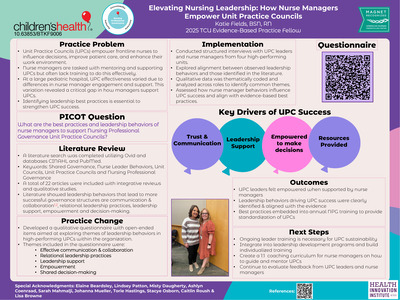
Elevating Nursing Leadership: How Nurse Managers Empower Unit Practice Councils
Katie Fields
EBP
Literature Review: Utilizing OVID and databases CINAHL and PubMed, a comprehensive review of 22 articles, including integrative reviews and qualitative studies, was conducted to examine leadership behaviors that support NPG and UPCs. Across the literature, empowerment, accountability, and presence are consistently highlighted as essential leadership behaviors for effective shared governance that strengthens engagement and professional growth. Clavelle and Tarasenko (2024) emphasized accountability as critical to advancing NPG, while Rollins et al. (2024) underscored the importance of adaptable leadership styles to meet the evolving needs of frontline nurses and practice councils.PICO: What are the best practices and leadership behaviors of nurse managers to support Nursing Professional Governance Unit Practice Councils
Evaluation: The evidence highlighted key behaviors such as effective communication and collaboration, relational leadership practices, leadership support, empowerment, and shared decision-making. To explore this alignment, a questionnaire of open-ended questions was created to uncover recurring leadership themes that support UPC success and sustainability. Using this tool, structured interviews were conducted with UPC leaders and nurse managers from four high-performing units to examine alignment between behaviors seen in practice and those identified in the literature. A consensus emerged regarding the leadership behaviors that contributed to UPC success. Relational leadership, consistent support, and shared decision-making were identified as key drivers of UPC effectiveness, aligning closely with the literature. UPC leaders consistently expressed that feeling supported and empowered by their nurse manager was crucial for their ability to lead.
-

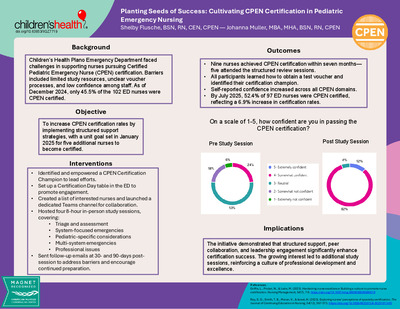
Planting Seeds of Success: Cultivating CPEN Certification in Pediatric Emergency Nursing
Shelby Flusche and Johanna Muller
INNOVATION & LEADERSHIP
Background: Children’s Health Plano campus has faced challenges in supporting nurses preparing for the Certified Pediatric Emergency Nurse (CPEN) exam, with limited resources available for study and preparation. To encourage certification, a certification champion was identified to provide leadership and guidance. However, it soon became evident that additional support was needed, as many nurses were unsure how to obtain a test voucher and reported low confidence levels regarding exam success. In fact, 75% of nurses initially rated themselves as neutral to not confident in their ability to pass the CPEN exam, highlighting a significant gap in preparedness and the need for structured educational and motivational strategies to improve certification outcomes. In December 2024 45.5% of the total 102 nurses within the Emergency Department were certified. A unit goal was made in January 2025 to have five nurses become certified with the changes made.Implementation: A list of nurses interested in pursuing their Certified Pediatric Emergency Nurse (CPEN) certification was obtained to identify participants. On certification day, an information table with a sign-up sheet for study review sessions was provided, generating strong engagement. A dedicated Microsoft Teams channel was created to foster communication and collaboration. Structured study sessions were held, with educational materials developed and presented by two experienced Registered Nurses (RN). A total of 11 nurses attended the first two review sessions. To sustain momentum, follow-up emails were distributed at 30 and 90 days post-session to encourage continued preparation and address barriers. Nurses who successfully achieved certification were recognized and celebrated, reinforcing a culture of professional growth and accomplishment.
Evaluation: In the first seven months, nine nurses achieved CPEN certification on their first attempt, with five attending an organized review session. All participants identified their certification champion and learned how to obtain a test voucher, reducing barriers to success. Nurses reported increased confidence, rating themselves as confident or very confident in triage, assessment, system-focused emergencies, special considerations, multi-system considerations, and professional issues. Growing demand led to two additional study sessions to support more nurses pursuing certification. These outcomes highlight the effectiveness of structured review sessions, leadership support, and peer collaboration. By July, 52.4% of 97 nurses in the Emergency Department were CPEN certified, demonstrating meaningful progress toward professional excellence.
-

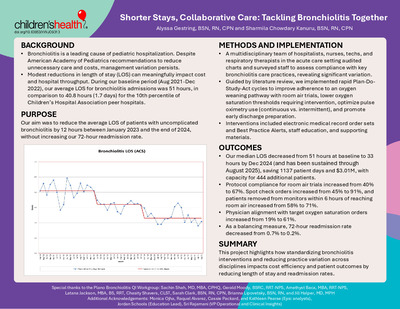
Shorter Stays, Collaborative Care: Tackling Bronchiolitis Together
Alyssa Gestring and Sharmila Chowdary Kanuru
QUALITY IMPROVEMENT
Background: Bronchiolitis is a leading cause of pediatric hospitalization. Despite American Academy of Pediatrics recommendations to reduce unnecessary care and costs, management variation persists. Modest reductions in length of stay (LOS) can meaningfully impact cost and hospital throughput. During our baseline period (Aug 2021-Dec 2022), our average LOS for bronchiolitis admissions was 51 hours, in comparison to 40.8 hours (1.7 days) for the 10th percentile of Children’s Hospital Association peer hospitals. Our aim was to reduce the average LOS of patients with uncomplicated bronchiolitis by 12 hours between January 2023 and the end of 2024, without increasing our 72-hour readmission rate.Methodology: A multidisciplinary team of hospitalists, nurses, techs, and respiratory therapists in the acute care setting audited charts and surveyed staff to assess compliance with key bronchiolitis care practices, revealing significant variation. Guided by literature review, we implemented rapid Plan-Do-Study-Act cycles to improve adherence to an oxygen weaning pathway with room air trials, lower oxygen saturation thresholds requiring intervention, optimize pulse oximetry use (continuous vs. intermittent), and promote early discharge preparation. Interventions included electronic medical record order sets and Best Practice Alerts, staff education, and supporting materials.
Outcomes: Our median LOS decreased from 51 hours at baseline to 33 hours by Dec 2024 and has been sustained through August 2025. Protocol compliance for room air trials increased from 40% to 67%. Spot check orders increased from 45% to 91%, and patients removed from monitors within 6 hours of reaching room air increased from 58% to 71%. Physician alignment with target oxygen saturation orders increased from 19% to 61%. As a balancing measure, 72-hour readmission rate decreased from 0.7% to 0.2%. In summary, this project highlights how standardizing nursing interventions and reducing practice variation impacts cost efficiency and patient outcomes by reducing length of stay and readmission rates.
-
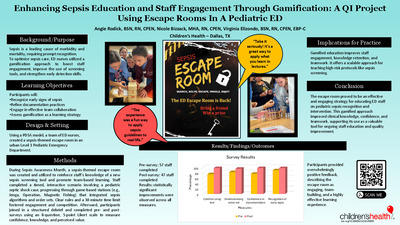
 Extravasation by Ann Gosdin, Hector Murillo, Taffi Marchand, and Brook Warren")
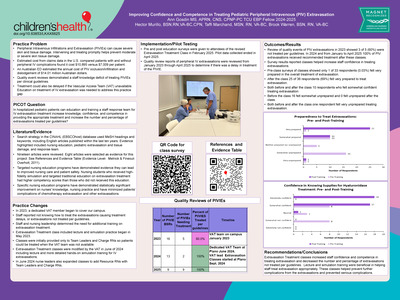
Improving Confidence and Competence in Treating Pediatric Peripheral Intravenous (PIV) Extravasation
Ann Gosdin, Hector Murillo, Taffi Marchand, and Brook Warren
EBP
Literature Review: Targeted nursing education has demonstrated it may lead to improved nursing care and patient safety. Nurses who received high-fidelity simulation and targeted traditional education on extravasation treatment had higher competency scores than those who did not received this education. Specific nursing education classes have demonstrated statistically significant improvement on nurses' knowledge, practice and minimized patients' complications of extravasations.PICO: In hospitalized pediatric patients can additional education and training by the Vascular Access Team (VAT) for Peripheral IV Infiltration and Extravasation (PIVIE) on extravasation treatment increase knowledge, confidence, and competence in providing the appropriate treatment and increase the percentage of extravasations treated per guidelines?
Evaluation: Staff reported not knowing how to treat the extravasations, causing treatment delays, or extravasations not being treated per guidelines. Staff and nursing leadership determined the need for additional training on Extravasation Treatment Informal education began in May 2023 to prepare nurses to treat patients when the VAT team wasn’t available. Classes were modified by VAT in June 2024 to include didactic lecture and simulation training for PIVIEs. Pre / post surveys were given to attendees of the revised class. Results: PIVIEs in 2023 showed 3 of 5 (60%) were not treated per guidelines. In 2024 and from January to April 2025 100% of PIVIEs received treatment. Pre-class surveys showed 1 of 33 respondents (0.03%) felt very prepared in overall treatment of PIVIE. After class 25 of 36 respondents (69%) felt very prepared to treat extravasation. Early treatment of extravasation minimized further complications.
-

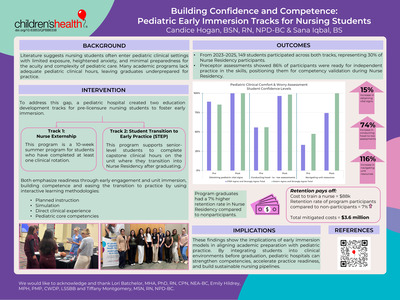
Building Confidence and Competence: Pediatric Early Immersion Tracks for Nursing Students
Candice Hogan and Sana Iqbal
INNOVATION & LEADERSHIP
Background: Literature suggests nursing students often enter pediatric clinical settings with limited exposure, heightened anxiety, and minimal preparedness for the acuity and complexity of pediatric care. Many academic programs lack adequate pediatric clinical hours, leaving graduates underprepared for practice. To address this gap, a pediatric hospital created two education development tracks for pre-licensure nursing students to foster early immersion.Implementation: Track one is a 10-week summer program for students who have completed at least one clinical rotation. Track two supports senior-level students to complete capstone clinical hours on the unit where they transition into Nurse Residency after graduating. Both emphasize readiness through early engagement and unit immersion, building competence and easing the transition to practice by using interactive learning methodologies. Each includes planned instruction, simulation, and direct clinical experience, aligned with pediatric core competencies for pre-licensure nurses. From 2023–2025, 149 students participated across both tracks, representing 30% of Nurse Residency participants. Educational outcomes were measured using pre- and post-program self-assessments adapted from a validated Pediatric Nursing Student Clinical Comfort and Worry Assessment Tool.
Evaluation: Students reported a 15% increase in confidence obtaining pediatric vital signs, a 74% increase in conducting head-to-toe assessments, and a 116% increase in navigating unit resources. Preceptor assessments showed 86% of participants were ready for independent practice in these skills, positioning them for competency validation during Nurse Residency. Beyond educational gains, program graduates had a 4% higher retention rate in Nurse Residency compared to non-participants. With an estimated $88,000 to train a new nurse, these outcomes represent $1.8 million in mitigated turnover costs. These findings show the implications of early immersion models in aligning academic preparation with pediatric practice. By integrating students into clinical environments before graduation, pediatric hospitals can strengthen competencies, accelerate practice readiness, and build sustainable nursing pipelines.
-

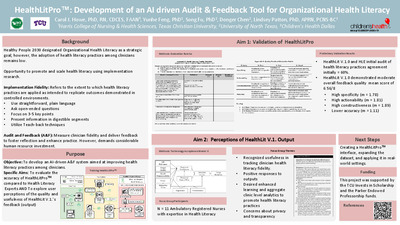
HealthLitPro™: Development of an AI driven Audit & Feedback Tool for Organizational Health Literacy
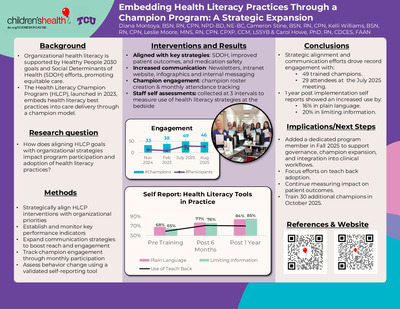
Carol J. Howe, Yunhe Feng, Song Fu, Donger Chen, and Lindsey Patton
RESEARCH
Purpose: Organizational Health Literacy (OHL) refers to the ability of healthcare institutions to support patients and families to access, understand, and use health information. Nurses play a key role in OHL using evidence-based health literacy practices (i.e. plain language, teach-back, open-ended questions, chunking information, and three to five key points) when educating patient families. Yet, implementation is challenging. Audit and Feedback (A&F) is an implementation strategy for promoting fidelity to health literacy practices. Conventionally requiring expert human evaluations that are costly, labor-intensive, and difficult to scale.
Methods: HealthLit was trained using a dataset of simulated nurse-patient education encounters and applies natural language processing, machine learning, and retrieval-augmented generation to evaluate fidelity to health literacy practices. The team refined the model through HLEs’ feedback and prompt engineering, enhancing contextual understanding and precision. HealthLit’s performance was validated using an adapted AHRQ Communication Observation Form to rate the presence of plain language, teach-back, and open-ended questions on a 0-2 scale (0 = absent, 1 = partially present, 2 = present). Feedback Quality Evaluation assessed specificity, actionability, constructiveness, accuracy on a 0-2 scale, with higher scores indicated better feedback quality. A focus group of 11 clinical nurses with training in health literacy provided feedback on the perceived usefulness and acceptability of outputs for further refinement.Results: A dataset of 33 nurse-patient transcripts was used for the model demonstrating moderate overall quality scores with a mean feedback quality score of 6.56/8 suggesting that while its feedback is somewhat helpful, it occasionally lacks details, specificity, and accuracy. The model demonstrated high specificity (m = 1.78), actionability (m = 1.81), and constructiveness (m = 1.89), but required improvement in accuracy over health literacy practices (m = 1.11). It was most accurate for open-ended questions (m = 1.22). It aligned closely with the health literacy expert evaluators across all health literacy practices in terms of actionability (m= 1.78 to 2) and constructiveness (m = 1.78 to 2). Focus group findings revealed key themes: positive response to HealthLit outputs and a desire for enhanced learning and analytics. Nurses recognized the usefulness in tracking health literacy fidelity and wished for case-based learning and aggregate clinic-level analytics.
-

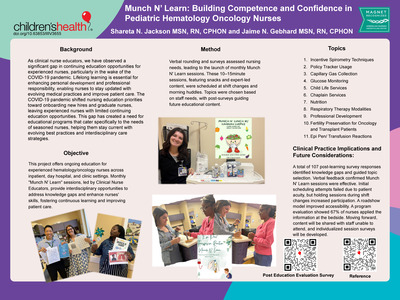
Munch N’ Learn: Building Competence and Confidence in Pediatric Hematology Oncology Nurses
Shareta N. Jackson and Jaime N. Gebhard
INNOVATION & LEADERSHIP
Background: As clinical nurse educators, we have observed a significant gap in continuing education opportunities for experienced nurses, particularly in the wake of the COVID-19 pandemic. Lifelong learning is essential for enhancing personal development and professional responsibility, enabling nurses to stay updated with evolving medical practices and improve patient care. The COVID-19 pandemic shifted nursing education priorities toward onboarding new hires and graduate nurses, leaving experienced nurses with limited continuing education opportunities. This gap has created a need for educational programs that cater specifically to the needs of seasoned nurses, helping them stay current with evolving best practices and interdisciplinary care strategies.Implementation: This project offers ongoing education for experienced hematology/oncology nurses across inpatient, day hospital, and clinic settings. Monthly "Munch N' Learn" sessions, led by Clinical Nurse Educators, provide interdisciplinary opportunities to address knowledge gaps and enhance nurses' skills, fostering continuous learning and improving patient care. Verbal rounding and surveys assessed nursing needs, leading to the launch of monthly Munch N' Learn sessions. These 10–15minute sessions, featuring snacks and expert-led content, were scheduled at shift changes and morning huddles. Topics were chosen based on staff needs, with post-surveys guiding future educational content.
Evaluation: A total of 107 post-learning survey responses identified knowledge gaps and guided topic selection. Verbal feedback confirmed Munch N' Learn sessions were effective. Initial scheduling attempts failed due to patient acuity, but holding sessions during shift changes increased participation. A roadshow model improved accessibility. A program evaluation showed 67% of nurses applied the information at the bedside. Moving forward, content will be shared with staff unable to attend, and individualized session surveys will be developed.
-

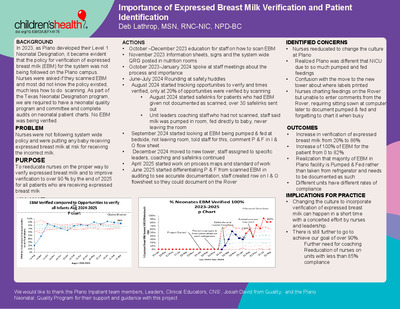
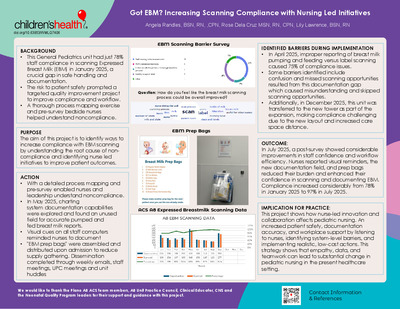
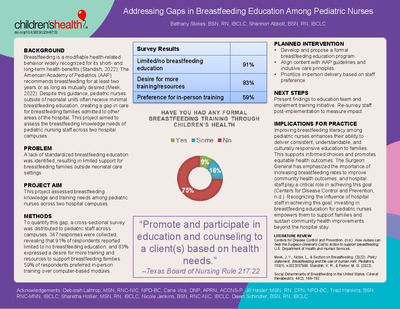
Importance of Expressed Breast Milk Verification and Patient Identification
Deb Lathrop
QUALITY IMPROVEMENT
Background: Due to changes in Texas reimbursement, the Plano campus was transferring neonates, infants under 28 days of life, to the Dallas campus. It was decided in 2023 to obtain a neonatal designation for the Plano campus. A Program Manager was hired as part of the requirements and a quality and Patient Safety committee was formed. As part of the program, quality data collection was required. As a Level I designated facility, expressed breastmilk verification was one of the required data sets to be collected. It was discovered that staff at the Plano campus were not scanning expressed breast milk(EBM). Of the over 100 nurses who attended neonatal classes, only 3 said they had ever scanned EBM at the Plano campus. Each of these three described a different process and none of them were correct when looking at the policy on Breast Milk Administration. With this information, we realized we must improve our process.Methodology: Due to changes in Texas reimbursement, the Plano campus was transferring neonates, infants under 28 days of life, to the Dallas campus. It was decided in 2023 to obtain a neonatal designation for the Plano campus. A Program Manager was hired as part of the requirements and a quality and Patient Safety committee was formed. As part of the program, quality data collection was required. As a Level I designated facility, expressed breastmilk verification was one of the required data sets to be collected. It was discovered that staff at the Plano campus were not scanning expressed breast milk(EBM). Of the over 100 nurses who attended neonatal classes, only 3 said they had ever scanned EBM at the Plano campus. Each of these three described a different process and none of them were correct when looking at the policy on Breast Milk Administration. With this information, we realized we must improve our process.
Outcomes:
- Verification rates increased from 20 % to over 90% hospital wide.
- Units had different rates, we will work on different strategies for following policy with each unit.
-

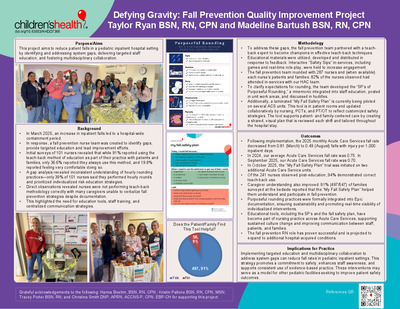
I Don’t Want to be Alone: The Impact of Cohorting Neonates on One Unit
Deb Lathrop and Rose Dela Cruz
INNOVATION & LEADERSHIP
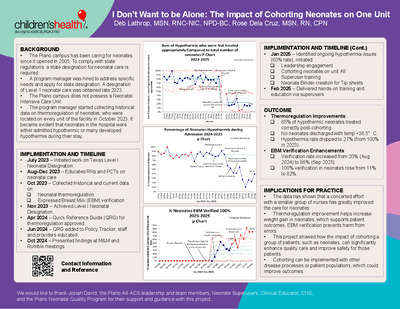
Background: The hospital has been caring for neonates since it opened in 2005. To comply with state regulations, a state designation for neonatal care is required. The facility hired a program manager to address specific needs and to apply for the state designation. A designation of Level 1 neonatal care was obtained at the end of 2023. The facility does not possess a Neonatal Intensive Care Unit. The program manager started collecting historical data on thermoregulation who are located on every unit of the facility in October 2023. It became evident that neonates in the hospital were either admitted hypothermic or developed hypothermia during their stay.Implementation:
- July 2023, Started working on Texas Designation for Level I
- Aug - Dec 2023, education RNs and PCTs on neonatal hypothermia presentations at staff meetings and safety huddles
- Apr 2024, QRG thermoregulation of neonates at Plano approved by MD, nursing channels
- Jun 2024, QRG in Policy Tracker, educated staff and providers to protocol
- Oct 2024, presented case in Plano M & M, Rumble meetings
- Jan 2025, still at 60% neonates hypothermic and most not being treated per protocol
- Met with hospital leadership, started cohorting neonates on A8
- Trained superusers
- Binder created
- Feb 2025, hands on training, education by superusers to staff
Evaluation:
- The impact of the initiative was dramatic
- July 2025, the percentage of neonates becoming hypothermic in the hospital decreased from 80% to 9%
- Most only became mildly hypothermic, between 36.0 – 36.4 C
- The percentage of neonates not treated per protocol dropped from 90% to less than 10%
The data has shown that a concerted effort with a smaller group of nurses has greatly improved the care for neonates. Thermoregulation improvement helps increase weight gain in neonates, which supports patient outcomes. This project showed how the impact of cohorting a group of patients, such as neonates, can significantly enhance quality care and improve safety for those patients. Cohorting can be implemented with other disease processes or patient populations, which could improve outcomes.
-

Blinatumomab Without Borders: Taking Life-saving Treatment Home
Susan McCollom, Tami Beaudin, Shareta Jackson, and Jamie Gebhard
INNOVATION & LEADERSHIP
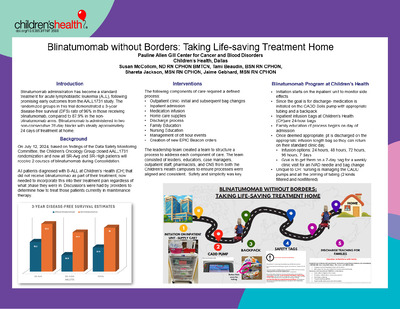
Background: Blinatumomab administration has become a standard treatment for acute lymphoblastic leukemia (ALL), following promising early outcomes from the AALL1731 study. The randomized groups in this trial demonstrated a 3-year disease-free survival (DFS) rate of 96% in those receiving blinatumomab, compared to 87.9% in the non-blinatumomab arms. Blinatumomab is administered in two non-consecutive 28-day blocks with ideally approximately 24 days of treatment at home.Implementation: The staff at the Center for Cancer and Blood Disorders (CCBD) at Children’s Health faced a significant challenge due to the volume and urgency of the therapy to start. We had about 44 patients needing 2 courses over the next 4 months. Nursing leadership brought together key stakeholders in nursing and pharmacy to analyze the various components required to safely discharge patients home on a continuous infusion and educate nursing on their role in the process. A challenge was obtaining organizational approval to initiate the infusion using a home care infusion pump that would be unique to our department. This was crucial to ensure a smooth transition for patients and their families, allowing them to receive treatment at home while being fully prepared for what to expect. Additional challenges included managing unexpected events during home infusions, such as pump malfunctions or tubing disconnections. Pharmacy’s support was needed to ensure safe handling of Blinatumomab.
Evaluation: From July 20, 2024 to December 31, 2024 CCBD initiated 74 inpatient Blinatumomab infusions and completed 237 bag changes across 2 campuses. We had 32 events that were related to pump, tubing or line issues that were unplanned with most of them occurring during off hours. In 2025, we added an addition 17 infusions in 7 months and anticipate more patients to receive this medication as it is added to more treatment protocols. As patients are newly diagnosed with ALL the process is embedded in our culture and has become standard of care.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}